Summary
Background
The early clinical course of COVID-19 can be difficult to distinguish from other illnesses driving presentation to hospital. However, viral-specific PCR testing has limited sensitivity and results can take up to 72 h for operational reasons. We aimed to develop and validate two early-detection models for COVID-19, screening for the disease among patients attending the emergency department and the subset being admitted to hospital, using routinely collected health-care data (laboratory tests, blood gas measurements, and vital signs). These data are typically available within the first hour of presentation to hospitals in high-income and middle-income countries, within the existing laboratory infrastructure.
Methods
We trained linear and non-linear machine learning classifiers to distinguish patients with COVID-19 from pre-pandemic controls, using electronic health record data for patients presenting to the emergency department and admitted across a group of four teaching hospitals in Oxfordshire, UK (Oxford University Hospitals). Data extracted included presentation blood tests, blood gas testing, vital signs, and results of PCR testing for respiratory viruses. Adult patients (>18 years) presenting to hospital before Dec 1, 2019 (before the first COVID-19 outbreak), were included in the COVID-19-negative cohort; those presenting to hospital between Dec 1, 2019, and April 19, 2020, with PCR-confirmed severe acute respiratory syndrome coronavirus 2 infection were included in the COVID-19-positive cohort. Patients who were subsequently admitted to hospital were included in their respective COVID-19-negative or COVID-19-positive admissions cohorts. Models were calibrated to sensitivities of 70%, 80%, and 90% during training, and performance was initially assessed on a held-out test set generated by an 80:20 split stratified by patients with COVID-19 and balanced equally with pre-pandemic controls. To simulate real-world performance at different stages of an epidemic, we generated test sets with varying prevalences of COVID-19 and assessed predictive values for our models. We prospectively validated our 80% sensitivity models for all patients presenting or admitted to the Oxford University Hospitals between April 20 and May 6, 2020, comparing model predictions with PCR test results.
Findings
We assessed 155 689 adult patients presenting to hospital between Dec 1, 2017, and April 19, 2020. 114 957 patients were included in the COVID-negative cohort and 437 in the COVID-positive cohort, for a full study population of 115 394 patients, with 72 310 admitted to hospital. With a sensitive configuration of 80%, our emergency department (ED) model achieved 77·4% sensitivity and 95·7% specificity (area under the receiver operating characteristic curve [AUROC] 0·939) for COVID-19 among all patients attending hospital, and the admissions model achieved 77·4% sensitivity and 94·8% specificity (AUROC 0·940) for the subset of patients admitted to hospital. Both models achieved high negative predictive values (NPV; >98·5%) across a range of prevalences (≤5%). We prospectively validated our models for all patients presenting and admitted to Oxford University Hospitals in a 2-week test period. The ED model (3326 patients) achieved 92·3% accuracy (NPV 97·6%, AUROC 0·881), and the admissions model (1715 patients) achieved 92·5% accuracy (97·7%, 0·871) in comparison with PCR results. Sensitivity analyses to account for uncertainty in negative PCR results improved apparent accuracy (ED model 95·1%, admissions model 94·1%) and NPV (ED model 99·0%, admissions model 98·5%).
Interpretation
Our models performed effectively as a screening test for COVID-19, excluding the illness with high-confidence by use of clinical data routinely available within 1 h of presentation to hospital. Our approach is rapidly scalable, fitting within the existing laboratory testing infrastructure and standard of care of hospitals in high-income and middle-income countries.
Funding
Wellcome Trust, University of Oxford, Engineering and Physical Sciences Research Council, National Institute for Health Research Oxford Biomedical Research Centre.
Evidence before this study
A detailed systematic review identified 91 diagnostic models for COVID-19 as of July 1, 2020; however, all were appraised to be at “high risk of bias”. Existing early detection models overwhelmingly consider radiological imaging (60 of 91 models), such as CT, which is less readily available than blood tests and involves exposure of patients to ionising radiation. Few studies assessed routine laboratory tests, with the scarce literature considering small numbers of patients with confirmed COVID-19 (<180), labelling patients as negative by use of the imperfectly sensitive PCR test and thereby failing to ensure disease freedom, inadequately accounting for breadth of alternative disease, and not being prospectively validated. No published studies considered whether laboratory artificial intelligence models can be applied to a clinical population as a screening test for COVID-19.
Added value of this study
To our knowledge, this was the largest laboratory artificial intelligence study on COVID-19 to date, training with clinical data from more than 115 000 patients presenting to hospital, and the first to integrate laboratory blood tests with point-of-care measurements of blood gases and vital signs. The breadth of our pre-pandemic control cohort exposed our classifiers to a wide variety of alternative illnesses and offered confidence that control patients did not have COVID-19. Here, we developed context-specific models for patient populations attending the emergency department and being admitted to hospital, and we showed clinically minded calibration by selecting for high negative predictive values at high classification performance. In doing so, we developed an effective screening test for COVID-19 using clinical data that are routinely acquired for patients presenting to hospital in the UK and typically available within 1 h. By simulating performance of our screening test at different stages of a pandemic, we showed high negative predictive values (>98·5%) when disease prevalence is low (≤5%), safely and rapidly excluding COVID-19. We prospectively validated our models by applying them to all patients presenting and admitted to the Oxford University Hospitals in a 2-week test period, achieving high accuracy (>92%) compared with PCR results.
Implications of all the available evidence
Rapid and accurate detection of COVID-19 in hospital admissions is essential for patient safety. Well described limitations of the current gold-standard test include turnaround times up to 72 h (as of July, 2020), limited sensitivity of about 70%, and shortages of skilled operators and reagents. The benefits of our artificial intelligence screening test are that it is immediately deployable at low cost, fits within existing clinical pathways and laboratory testing infrastructure, gives a result within 1 h that can safely exclude COVID-19, and ensures that patients can receive upcoming treatments rapidly.
Introduction
The early clinical course of COVID-19, which often includes common symptoms such as fever and cough, can be challenging for clinicians to distinguish from other respiratory illnesses.
,
,
,
,
These include limited sensitivity,
,
a long turnaround time of up to 72 h, and requirements for specialist laboratory infrastructure and expertise.
Studies have shown a significant proportion of asymptomatic carriage and limited specificity for common symptoms (fever and cough), hampering symptom-guided hospital triage.
Therefore, an urgent clinical need exists for rapid, point-of-care identification of COVID-19 to support expedient delivery of care and to assist front-door triage and patient streaming for infection control purposes.
,
Basic laboratory blood tests and physiological clinical measurements (vital signs) are among the routinely collected health-care data typically available within the first hour of presentation to hospitals in high-income and middle-income countries, and patterns of changes have been described in retrospective observational studies of patients with COVID-19 (variables including lymphocyte count, and alanine aminotransferase, C-reactive protein [CRP], D-dimer, and bilirubin concentrations).
,
,
,
Moreover, previous health-care data available in the EHR might be useful in identifying risk factors for COVID-19 or underlying conditions that might cause alternative, but similar, presentations.
In this study, we applied artificial intelligence methods to a rich clinical dataset to develop and validate a rapidly deployable screening model for COVID-19. Such a tool would facilitate rapid exclusion of COVID-19 in patients presenting to hospital, optimising patient flow and serving as a pretest where access to confirmatory molecular testing is limited.
Methods
Data collection
Linked deidentified demographic and clinical data for all patients presenting to emergency and acute medical services at Oxford University Hospitals (Oxford, UK) between Dec 1, 2017, and April 19, 2020, were extracted from EHR systems. Oxford University Hospitals consist of four teaching hospitals, serving a population of 600 000 and providing tertiary referral services to the surrounding region.
For each presentation, data extracted included presentation blood tests, blood gas testing, vital signs, results of RT-PCR assays for SARS-CoV-2 (Abbott Architect [Abbott, Maidenhead, UK], and Public Health England-designed RNA-dependent RNA polymerase) from nasopharyngeal swabs, and PCR for influenza and other respiratory viruses. Where available, the following baseline health data were included: the Charlson comorbidity index, calculated from comorbidities recorded during a previous hospital encounter since Dec 1, 2017 (if any existed); and changes in blood test values relative to pre-presentation results. Patients who had opted out of EHR research, did not receive laboratory blood tests, or were younger than 18 years were excluded from analysis. Analyses were confined to clinical, laboratory, and historical data routinely available within the first hour of presentation to hospital.
Adult patients presenting to hospital before Dec 1, 2019, and thus before the global outbreak, were included in the COVID-19-negative cohort. A subset of this cohort was admitted to hospital and included in the COVID-19-negative admissions cohort. Patients presenting to hospital between Dec 1, 2019, and April 19, 2020, with PCR-confirmed SARS-CoV-2 infection were included in the COVID-19-positive cohort, with the subset admitted to hospital included in the COVID-19-positive admissions cohort. Because of incomplete penetrance of testing during early stages of the pandemic and limited sensitivity of the PCR swab test, there is uncertainty in the viral status of patients presenting during the pandemic who were untested or tested negative. Therefore, these patients were excluded from the analysis.
The study protocol, design and data requirements were approved by the National Health Service (NHS) Health Research Authority (IRAS ID 281832) and sponsored by the University of Oxford.
Feature sets
We computed changes in blood tests from previous laboratory samples taken at least 30 days before presentation to hospital (available from Dec 1, 2017, onwards).
Table 1Clinical parameters included in each feature set
ALT=alanine aminotransferase. APTT=activated partial thromboplastin time. CRP=C-reactive protein. eGFR=estimated glomerular filtration rate. INR=international normalised ratio. p50=pressure at which haemoglobin is 50% bound to oxygen.
Model training, calibration, and testing
,
were trained to distinguish patients presenting or admitted to hospital with confirmed COVID-19 from pre-pandemic controls. We developed separate models to predict COVID-19 in all patients attending the emergency department (ED model) and then in the subset of those who were subsequently admitted to hospital (admissions model).
Table 2Population characteristics for the study cohorts and the prospective validation set
Data are n (%) or median (IQR). EHR=electronic health-care record.
We assessed performance of each configuration using the held-out test set. First, we configured the test set with equal numbers of COVID-19 cases and pre-pandemic controls, ensuring that performance was assessed in conditions free of class imbalance, and reported AUROC alongside sensitivity and specificity at each threshold. Second, to simulate model performance at varying stages of the pandemic, we generated a series of test sets with various prevalences of COVID-19 (1–50%) by use of the held-out set. We report positive and negative predictive values for each model at the 70% and 80% sensitivity thresholds. AUROC, sensitivity, specificity, and precision are reported for candidate models at the described thresholds. Positive predictive values (PPVs) and negative predictive values (NPVs) are reported for the simulated test sets. To understand the contribution of individual features to model predictions, we queried importance scores and did SHAP (Shapley additive explanations) analysis.
Validation
Models were validated independently by use of data for all adult patients presenting or admitted to Oxford University Hospitals between April 20 and May 6, 2020, by direct comparison of model prediction against SARS-CoV-2 PCR results. Because of incomplete penetrance of testing and limited sensitivity of the PCR swab test, we did a sensitivity analysis to ensure disease freedom in patients labelled as COVID-19 negative during validation, replacing patients who tested negative by PCR assay or who were not tested with truly negative pre-pandemic patients matched for age, gender, and ethnicity. Accuracy, AUROC, NPV, and PPV were reported during validation. We assessed rates of misclassification by characteristics of age, gender, and ethnicity; comparison between groups was done with Fishers’ exact test. We used the SciPy library for Python, version 1.2.3.
Role of the funding source
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the manuscript. All authors had full access to all the data in the study. AASS and SK guarantee the data and analysis. The corresponding author had final responsibility for the decision to submit for publication.
Results
Table 3AUROCs achieved for each independent feature set and for increasing feature sets using stratified 10-fold cross-validation during training
Data are AUROC (SD). Δ=change in results from baseline. AUROC=area under the receiver operating characteristic curve. CCI=Charlson comorbidity index.
Table 4Assessment of performance of the ED and admissions models, calibrated to 70%, 80%, and 90% sensitivities during training, in identifying COVID-19 in patients presenting to or admitted to hospital in the held-out test set
Data are performance (SD). The test set was generated from an 80:20 stratified train-test split of the dataset and balanced equally with controls (50% assumed prevalence). AUROC=area under the receiver operating characteristic curve. ED=emergency department. NPV=negative predictive values. PPV=positive predictive values.

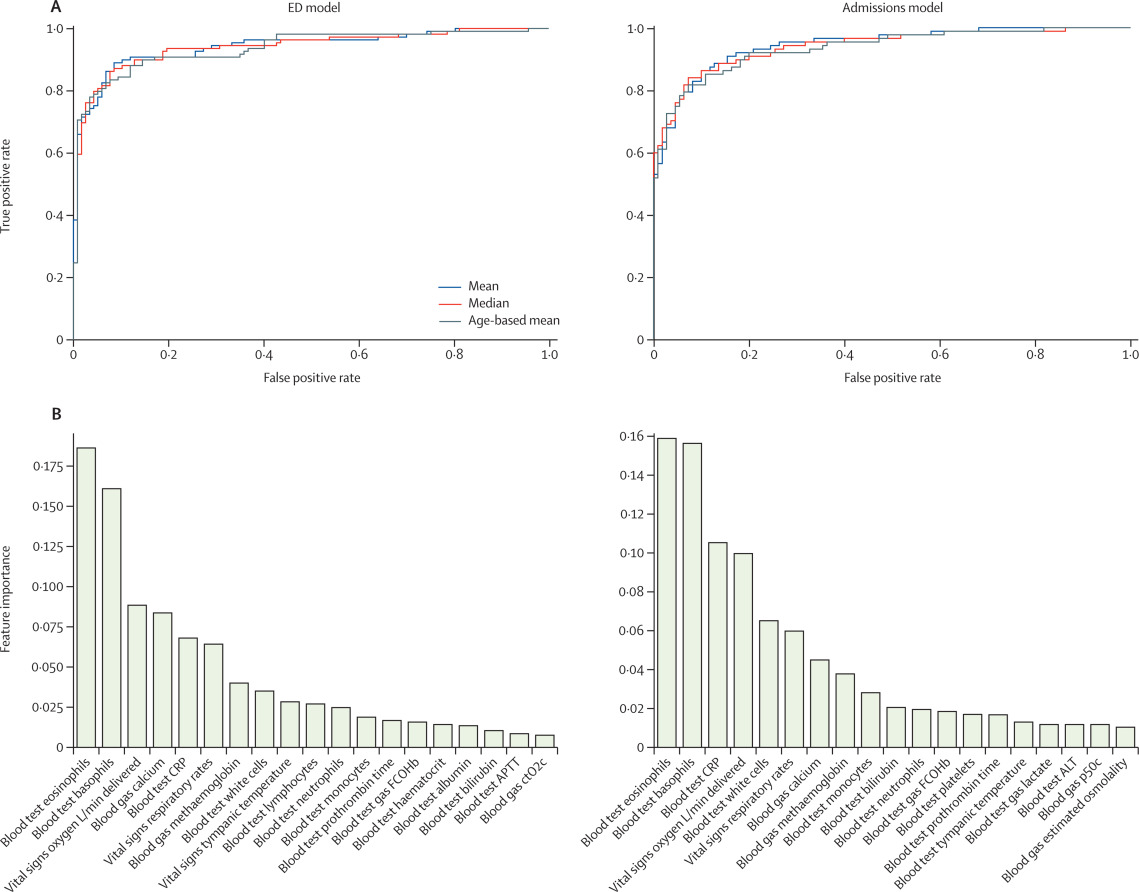
FigureReceiver operating characteristic curves (A) and relative importance of features (B) for the ED and admissions models
ALT=alanine aminotransferase. APTT=activated partial thromboplastin time. CRP=C-reactive protein. ctO2c=calculated oxygen content. ED=emergency department. FCOHb=fraction of carboxyhaemoglobin. p50c=calculated pressure at which haemoglobin is 50% bound to oxygen.
Table 5PPV and NPV of the ED and admissions models, calibrated during training to 70% and 80% sensitivities, for identifying COVID-19 in test sets with various prevalences
ED=emergency department. NPV=negative predictive values. PPV=positive predictive values.
We prospectively validated our ED and admissions models, calibrated during training to 80% sensitivity, for all patients presenting or admitted to Oxford University Hospitals between April 20 and May 6, 2020. 3326 patients presented to hospital and 1715 were admitted during the validation period. Prevalences of COVID-19 were 3·2% (107 of 3326) in patients presenting to hospital and 5·3% (91 of 1715) in those admitted to hospital. Our ED model performed with 92·3% accuracy (AUROC 0·881) and the admission model performed with 92·5% accuracy (0·871) on the validation set, assessed against results of laboratory PCR testing. PPVs were 46·7% (ED model) and 40·0% (admissions model) and NPVs were 97·6% (ED) and 97·7% (admissions).
We did a sensitivity analysis to account for uncertainty in the viral status of patients testing negative by PCR or who were not tested. Our ED model showed an apparent improvement in accuracy to 95·1% (AUROC 0·960) and our admission model improved to 94·1% accuracy (0·937) on the adjusted validation set. NPVs achieved were also improved to 99·0% (ED model) and 98·5% (admissions model).
To assess model performance on clinically important subgroups, we assessed performance of our admissions model on patients presenting during prospective validation who went on to require admission to the intensive care unit (ICU) or who died. The model performed highest on the subpopulation admitted to ICU (AUROC 0·930, accuracy 93·5%, NPV 98·3%, PPV 37·8%) and also achieved high performance for patients who died during admission (0·916, accuracy 93·0%, NPV 98·3%, PPV 37·6%). Additionally, we investigated model performance for the subset of patients presenting with respiratory symptoms, showing high performance for this key group (0·895, accuracy 92·8%, NPV 98·0%, PPV 35·6%).
To evaluate for biases in model performance, we assessed rates of patient misclassification during validation of our ED and admissions models. We observed that rates of misclassification were similar between White British (ED model 9%, admissions model 10%) and Black, Asian, and minority ethnic group patients (ED 11%, admissions 13%; Fishers’ exact test p=0·37 for ED and p=0·36 for admissions), and between men (11% for both models) and women (8% for both models; p=0·15 for ED and p=0·091 for admissions). We also found no difference between misclassification of patients older than 60 years (10% for both models) and patients aged 18–60 years (9% ED model and 8% admissions model; p=0·19 for ED and admissions).
Discussion
shortages of specialist equipment and operators, and relatively low sensitivity.
NHS guidelines require testing of all emergency admissions,
irrespective of clinical suspicion, highlighting the demand for rapid and accurate exclusion of COVID-19 in the acute care setting.
In this study, we developed and assessed two context-specific artificial intelligence-driven screening tools for COVID-19. Our ED and admissions models effectively identified patients with COVID-19 among all patients presenting and admitted to hospital, using data typically available within the first hour of presentation. Simulation on test sets with varying prevalences of COVID-19 showed that our models achieved clinically useful NPVs (>98·5%) at low prevalences (≤5%). On validation, using prospective cohorts of all patients presenting or admitted to the Oxford University Hospitals, our models achieved high accuracies and NPVs compared with PCR test results. A sensitivity analysis to account for uncertainty in negative PCR results improved apparent accuracy and NPVs.
The strengths of our artificial intelligence approach include an ability to scale rapidly, taking advantage of cloud computing platforms and working with laboratory tests widely available and routinely done within the current standard of care. Moreover, we showed that our models can be calibrated to meet changing clinical requirements at different stages of the pandemic, such as a high PPV model.
,
,
,
which is less readily available and involves patient exposure to ionising radiation. Few studies have assessed routine laboratory tests, with studies to date including small numbers of patients with confirmed COVID-19, using PCR results for data labelling and thereby not ensuring disease freedom in so-called negative patients and not being validated in the clinical population that is the target for their intended use.
,
,
A substantial limitation of existing works is the use of narrow control cohorts during training, inadequately exposing models to the breadth and variety of alternative infectious and non-infectious pathologies, including seasonal pathologies. Moreover, although the use of artificial intelligence techniques for early detection holds great promise, many published models to date have been assessed to be at high risk of bias.
Our study includes the largest dataset of any laboratory artificial intelligence study on COVID-19 to date, considering over 115 000 hospital attendances and 5 million measurements, and it is prospectively validated with use of appropriate patient cohorts for the models’ intended clinical contexts. The breadth of our pre-pandemic control cohort gives exposure to a wide range of undifferentiated presentations, including other seasonal infectious pathologies (eg, influenza), and offers confidence in SARS-CoV-2 freedom. Additionally, to our knowledge, our study is the first to integrate laboratory blood results with blood gas and vital signs measurements taken at presentation to hospital, maximising the richness of the dataset available.
We selected established linear and non-linear modelling approaches, achieving highest performance with XGBoost, an extreme gradient boosted tree method. Information variables from all sets were important in model predictions, including three measured biochemical quantities (eosinophils, basophils, and CRP), blood gas measurements (methaemoglobin and calcium), and vital signs (respiratory rate and oxygen delivery).
,
We observed that lymphopenia was frequently absent on first-available laboratory tests done on admission (appendix pp 3–4) and was not a highly ranked feature in our models (figure 1). Univariate analysis identified that eosinopenia on presentation was more strongly correlated with COVID-19 diagnosis than lymphocyte count (appendix p 6; χ2 score 41·61 for eosinopenia and 31·56 for lymphocyte count).
Recognising concerns of biases within artificial intelligence models, we assessed cases misclassified during validation for evidence of ethnicity, age, and gender biases. Our results showed misclassification was not significantly different between White British and Black, Asian, and minority ethnic patients; men and women; and older (>60 years) and younger (18–59 years) patients.
Our study seeks to address limitations common to EHR research. We used multiple imputations for missing data, taking a mean of three strategies (age-based imputation, population mean, and population median). We queried whether our results were sensitive to the imputation strategy and found similar model performance across the three strategies.
Additionally, as the first wave of COVID-19 cases in the UK largely followed the conclusion of the 2019–20 influenza season, data for patients who were co-infected were not available for this study.
,
Future work might examine a role for rapid screening in the paediatric population to reduce nosocomial transmission and assess model applicability in co-infection.
Our work shows that an artificial intelligence-driven screening test can effectively triage patients presenting to hospital for COVID-19 while confirmatory laboratory testing is pending. Our approach is rapidly scalable, fitting within the existing laboratory testing infrastructure and standard of care, and serves as proof of concept for a rapidly deployable software tool in future pandemics. Prospective clinical trials would further assess model generalisability and real-world performance.
Contributors
AASS, DAC, TZ, DWE, ZBH, and TP conceived of and designed the study. DWE extracted the data from EHR systems. TT, SK, and AASS pre-processed the data. DK, SK, AASS, TZ, TT, DWE, and DAC developed the models. AASS, SK, DK, TZ, AJB, DWE, and DAC validated the models. AASS, SK, and ZBH wrote the manuscript. DWE, TT, AASS, and SK had access to and verified the data. All authors revised the manuscript.
Declaration of interests
DWE reports personal fees from Gilead, outside the submitted work. DAC reports personal fees from Oxford University Innovation, BioBeats, and Sensyne Health, outside the submitted work. All other authors declare no competing interests.
Data sharing
Acknowledgments
We express our sincere thanks to all patients, clinicians, and staff across Oxford University Hospitals NHS Foundation Trust. We additionally thank staff across the University of Oxford Institute of Biomedical Engineering, Research Services, and Clinical Trials and Research Group. In particular, we thank Dr Ravi Pattanshetty for clinical input and Jia Wei. This research was supported by grants from the Wellcome Trust (University of Oxford Medical and Life Sciences Translational Fund, award 0009350), the Engineering and Physical Sciences Research Council (EP/P009824/1 and EP/N020774/1), and the NIHR Oxford Biomedical Research Centre and NIHR Health Protection Research Unit in Healthcare Associated Infections and Antimicrobial Resistance at the University of Oxford (NIHR200915), in partnership with Public Health England (PHE). AASS is an NIHR Academic Clinical Fellow. DWE is a Robertson Foundation Fellow and an NIHR Oxford Biomedical Research Centre Senior Fellow. The views expressed are those of the authors and not necessarily those of the NHS, NIHR, PHE, Wellcome Trust, or the Department of Health.
Supplementary Material
References
- 1.
Rolling updates on coronavirus disease (COVID-19).
- 2.
Novel coronavirus during the early outbreak period: epidemiology, causes, clinical manifestation and diagnosis, prevention and control.
Infect Dis Poverty. 2020; 9: 1-12
- 3.
Clinical characteristics of coronavirus disease 2019 in China.
N Engl J Med. 2020; 382: 1708-1720
- 4.
Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China.
JAMA. 2020; 323: 1061-1069
- 5.
Diagnosis of the coronavirus disease (COVID-19): rRT-PCR or CT?.
Eur J Radiol. 2020; 126108961
- 6.
Guidance and standard operating procedure: COVID-19 virus testing in NHS laboratories.
National Health Service,
London2020 - 7.
Occurrence and timing of subsequent SARS-CoV-2 RT-PCR positivity among initially negative patients.
Clin Infect Dis. 2020; ()
- 8.
The laboratory diagnosis of COVID-19 infection: current issues and challenges.
J Clin Microbiol. 2020; 58: 1-9
- 9.
Three quarters of people with SARS-CoV-2 infection are asymptomatic: analysis of English household survey data.
Clin Epidemiol. 2020; 12: 1039-1043
- 10.
Diagnosing COVID-19: the disease and tools for detection.
ACS Nano. 2020; 14: 3822-3835
- 11.
Detection of COVID-19 infection from routine blood exams with machine learning: a feasibility study.
J Med Syst. 2020; 44: 135
- 12.
Real-time tracking of self-reported symptoms to predict potential COVID-19.
Nat Med. 2020; 26: 1037-1040
- 13.
Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement.
Ann Intern Med. 2015; 162: 55-63
- 14.
Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: prospective observational cohort study.
BMJ. 2020; 369m1985
- 15.
The role of biomarkers in diagnosis of COVID-19—a systematic review.
Life Sci. 2020; 254117788
- 16.
Routine blood tests are associated with short term mortality and can improve emergency department triage: a cohort study of >12,000 patients.
Scand J Trauma Resusc Emerg Med. 2017; 25: 115
- 17.
Chen T, Guestrin C. XGBoost: a scalable tree boosting system. KDD 19: The 25th ACM SIGKDD Conference on Knowledge Discovery and Data Mining; Anchorage, AK, USA; Aug 13–17, 2019.
- 18.
Scikit-learn.
GetMobile Mob Comput Commun. 2015; 19: 29-33
- 19.
Artificial intelligence-enabled rapid diagnosis of patients with COVID-19.
Nat Med. 2020; 26: 1224-1228
- 20.
Healthcare associated COVID-19 infections—further action.
- 21.
Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis.
N Engl J Med. 2003; 349: 1227-1235
- 22.
Prediction models for diagnosis and prognosis of COVID-19 infection: systematic review and critical appraisal.
BMJ. 2020; 369 m1328
- 23.
A fully automatic deep learning system for COVID-19 diagnostic and prognostic analysis.
Eur Respir J. 2020; 562000775
- 24.
A Novel triage tool of artificial intelligence assisted diagnosis aid system for suspected COVID-19 pneumonia in fever clinics.
SSRN. 2020; ()
- 25.
Epidemiological and clinical predictors of COVID-19.
Clin Infect Dis. 2020; 71: 786-792
- 26.
Hospitalization rates and characteristics of children aged <18 years hospitalized with laboratory-confirmed COVID-19—COVID-NET, 14 States, March 1-July 25, 2020.
MMWR Morb Mortal Wkly Rep. 2020; 69: 1081-1088
- 27.
Coronavirus (COVID-19) in the UK: dashboard.
- 28.
Weekly national flu reports: 2019 to 2020 season.
Article Info
Publication History
Published: December 11, 2020
Identification
Copyright
© 2020 The Author(s). Published by Elsevier Ltd.







{kind=link}