Depending on their training, upper extremity surgeons may perform a diverse set of operations, ranging from common hand surgeries to advanced microsurgery as well as shoulder and elbow arthroscopy and arthroplasty. Declining orthopedic reimbursement rates during the past two decades1 may encourage surgeons to shift their practice distribution toward procedures with higher compensation. In fact, a survey of newly graduated hand-fellowship applicants found a heavy demand for shoulder and elbow exposure, with 48% seeking such training.2 A second survey of hand-fellowship applicants echoed this, with 58% believing that shoulder and elbow exposure would be beneficial.3
One presumed notion among hand-fellowship applicants seeking such experience is that it adds increased “marketability” or financial success.4 To determine whether upper extremity surgeons and hand-fellowship trainees may be financially incentivized to perform more shoulder and elbow procedures over hand procedures, this study compared work relative value unit (wRVU) compensation rates for the most common procedures performed in a hospital-based setting between the 2 fields.
Materials and Methods
To determine the most common surgeries from each field, the authors analyzed isolated Current Procedural Terminology (CPT) codes tracked by the Accreditation Council for Graduate Medical Education performed in a facility (nonoffice) setting with volumes greater than 1000.5 After excluding CPT codes uniformly associated with orthopedic shoulder trauma, the authors identified 29 shoulder and elbow CPT codes. To identify the most common hand procedures, the authors included CPT codes for any orthopedic trauma distal to the elbow and any soft-tissue procedures distal to the shoulder, yielding 83 CPT codes.6
Actual “real-world” operative times (from skin incision to closure) were recorded from the National Surgical Quality Improvement Program (NSQIP). No entries for shoulder manipulation under anesthesia (23700) were present in NSQIP. After excluding subacromial decompression (29826) because it is no longer universally considered a stand-alone primary code, there were 27 shoulder and elbow codes for analysis. Because NSQIP only collects perioperative data for inpatient hospital-based hand surgery, routine outpatient elective hand surgeries, such as carpal tunnel release and trigger finger release, could not be included. This narrowed the analysis to 53 hand surgeries.
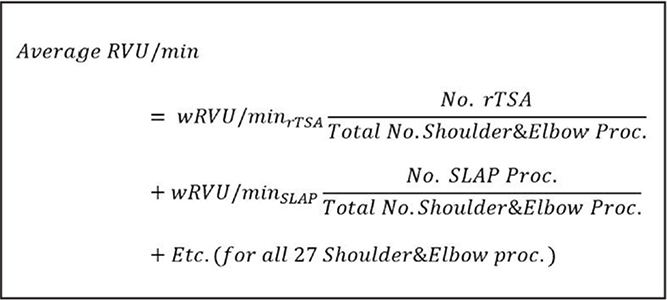
Compensation rates were determined by dividing each procedure wRVU by operative time to calculate compensation per minute. Compensation rates were analyzed in isolation (vs multiple codes per surgery) due to a high level of heterogeneity when determining whether additional procedures during a single surgery were considered bundled or not by different payers. Nonweighted and weighted overall wRVU/min averages for both fields were determined as well as average operative times. Weighted means were calculated according to the volume and frequency of each procedure divided by the total volume of all procedures performed (Figure 1). Both nonweighted and weighted Student t tests were used to determine whether there was a difference in compensation between the 2 fields.
 |
Figure 1: Equation—weighted relative value unit (wRVU) per minute for 27 shoulder and elbow procedures. In this equation, more commonly performed procedures will affect the mean wRVU/min more than less commonly performed procedures. This formula also was used to calculate the weighted RVU/min rate of all 53 hand procedures and average operative time of both fields. Abbreviations: Proc, procedure; rTSA, revision total shoulder arthroplasty; SLAP, arthroscopic superior labral tear from anterior to posterior repair. |
Results
For the 27 shoulder and elbow procedures analyzed, revision shoulder arthroplasty (23473) had the highest wRVU assignment as well as wRVU/min (Table A, available in the online version of the article). All but 2 of the top half of the highest earning procedures, in terms of RVU/min, consisted of arthroplasty, shoulder arthroscopy (superior labral tear from anterior to posterior repair, rotator cuff repair, capsulorrhaphy, biceps tenodesis, debridement, and lysis of adhesions), or open rotator cuff repair.
  |
Table A. wRVUs/min Rates based on NSQIP Operative Time for 27 of the Most Common Shoulder/Elbow CPT Codes, According to Centers for Medicare and Medicaid Services. |
Among the 53 hand and upper extremity procedure codes surveyed, upper extremity flaps (15736), carpal stabilization procedures (25320), distal radius open reduction and internal fixation for intraarticular comminuted fractures (25609), both-bone open reduction and internal fixation (25575), and interposition arthroplasty (25447) had the greatest wRVU assignments (Table B, available in the online version of the article). However, when factoring in operative time, none of these 5 procedures were compensated as well as the top 14 shoulder and elbow procedures (all ≥0.20 RVU/min). Only 7 of the 53 hand procedures earned 0.20 wRVU/min or greater.
  |
Table B. wRVUs/min Rates Based on NSQIP Operative Time for 53 of the Most Common Hosptial-based Hand Procedures, According to Centers for Medicare and Medicaid Services. |
Both nonweighted and weighted overall wRVU/min averages for shoulder and elbow surgery were greater than hospital-based hand surgery (P<.0001 for both) (Figure 2). The nonweighted average operative time was greater for shoulder and elbow surgery compared with hand surgery (65.9±27.5 min vs 55.0±21.6 min, P<.05) but similar when weighted for procedure frequency (63.9±21.5 min vs 56.9±20.7 min, P=.16). Although operative time remained unchanged across all shoulder and elbow surgeries surveyed when sorted by decreasing RVU/min (R=0.002; Figure 3), operative time tended to increase for lower-compensating hand procedures (R=0.5; Figure 4).
 |
Figure 2: Nonweighted and weighted (by surgical volume and frequency) average weighted relative value unit (wRVU) per minute compensation rates of 27 shoulder and elbow procedures and 53 hand procedures. Error bars show standard deviation; P<.0001 for nonweighted and weighted comparisons. |
 |
Figure 3: Weighted relative value unit (wRVU) per minute and operative times for 27 of the most common shoulder and elbow surgery Current Procedural Terminology codes. Secondary axis shows operative time (in red) with a linear regression trend line (R=0.002). Procedures sorted by descending wRVU/min rates. Abbreviations: CA, coracoacromial; SA, subacromial; SLAP, superior labral tear from anterior to posterior; TSA, total shoulder arthroplasty. |
 |
Figure 4: Weighted relative value unit (wRVU) per minute and operative times for 53 of the most common hand surgery Current Procedural Terminology codes. Secondary axis shows operative time (in red) with a linear regression trend line (R=0.5). Procedures sorted by descending wRVU/min rates. Note the upward trend of increased operative time for lower RVU/min cases, which is not observed in Figure 3. Abbreviations: CMC, carpometacarpal; EA, extra-articular; IA, intra-articular; IC, intercarpal; IPJ, interphalangeal joint; MC, metacarpal; MCPJ, metacarpal phalangeal joint; ORIF, open reduction and internal fixation; TFCC, triangular fibrocartilage complex. |
Discussion
In this analysis of wRVU compensation rates, nonweighted and weighted averages for hospital-based shoulder and elbow surgery were greater compared with hand surgery when using real-world NSQIP operative times. Half of the shoulder and elbow codes compensated the same or more than all but 2 hand procedures. In addition, when comparing operative times, average operative times were longer for shoulder and elbow procedures compared with hand procedures. Although this difference did not remain significant after weighting for procedure frequency, it suggests that total compensation from hand procedures can be more vulnerable to increased turnover time and to more frequent turnovers between shorter cases. This can be particularly problematic in operative settings where turnover time is relatively slower. Furthermore, the financial implications of these results may help explain the heavy preference for shoulder and elbow exposure among hand-fellowship trainees2,3 and corroborates other findings showing higher earning potential for shoulder and elbow-trained surgeons compared with hand-fellowship trained surgeons.7
Despite this stated preference for shoulder and elbow exposure among hand-fellowship trainees, the majority of hand-fellowship directors do not consider shoulder pathology as an essential competency for a hand-fellowship trainee. In a national survey of 62 fellowship directors, only 8% considered upper arm and shoulder conditions as an essential area of practice,8 suggesting that obtaining adequate exposure to shoulder and elbow elective experience may be a challenge for interested hand-fellowship trainees. This disconnect highlights the need to improve or redesign traditional fellowship programs to better serve trainees’ goals.
One factor that may explain higher compensation for shoulder and elbow procedures is that relatively newer CPT codes may be allotted higher RVU designations. The advent of shoulder arthroscopy is relatively recent and has generated several new CPT codes. In contrast, the vast majority of hand procedures are still based on open techniques without a notable expansion of CPT codes over the same time.
In an assessment of Medicare reimbursement for orthopedic procedures, relatively newer CPT codes, such as shoulder arthroscopy and decompression, were among the procedures that underwent the greatest mean annual decreases in reimbursement.1 On the other hand, procedures such as carpal tunnel saw the least annual reimbursement decrease. In 2012 after the Centers for Medicare & Medicaid Services changed arthroscopic acromioplasty (CPT 29826) from a stand-alone code to an add-on code, Medicare reimbursement dropped 36.3% during a 1-year period from 2011 to 2012.9 These studies suggest future periodic reevaluation of orthopedic CPT codes by the Centers for Medicare & Medicaid Services may narrow the compensation gap between the 2 fields.
There were limitations in the current analyses. One limitation in the authors’ methodology was not accounting for surgeries where multiple CPT codes were used. This practice can be particularly common in arthroscopic shoulder surgery, and accounting for this would likely further increase the overall wRVU averages for shoulder and elbow surgery. For example, CPT code 29823 (extensive arthroscopic debridement) may be routinely added to codes 29824 (distal claviculectomy), 23430/29828 (open/arthroscopic biceps tenodesis), 29827 (rotator cuff repair), and 29826 (subacromial decompression),10 which also are commonly grouped together during a single surgery when indicated.
However, add-on codes typically are reimbursed at diminished value under Medicare’s multiple code rule (eg, 50% for second code, 50% or 25% for third code, and beyond) because of shared operative preparation and approach. There is a large heterogeneity among different payers in how they reimburse multiple codes, with many insurers bundling procedures under a parent code. Furthermore, because the current analysis used wRVU compensation rates per minute of operative time instead of total wRVU collected per case, the benefits of multiple codes was minimized. For example, adding on a mini-open biceps tenodesis requires a separate incision and additional separate work during the diagnostic arthroscopy.
Other limitations included an inability to completely capture all procedures performed in each field. Some shoulder and elbow codes were not accounted for, such as open Bankart repair (23455) or a superior capsular reconstruction (29999, unlisted procedure). Similarly, some hand procedure codes, including all replants, which have high RVU assignments but are generally lengthy cases, were not included in this study due to low volume. However, not all upper extremity and hand surgeons perform these types of surgeries, and the low volumes at which these surgeries are performed would not likely significantly affect the overall averages.
The current analysis also did not account for postoperative care and work in the 90-day global period, although these aspects are factored into the wRVU calculations. Because most upper extremity procedures require some form of postoperative immobilization, wound check, and physical therapy, postoperative care and physician effort are likely similar between the 2 fields. Finally, the case volume and frequencies used to compute the weighted means are based on Medicare populations and may shift depending on the patient population of the treating surgeon.
Conclusion
Hospital-based shoulder and elbow procedures compensate significantly higher wRVU rates per operative time compared with hand surgery. These findings have important implications for both providers and hand-fellowship trainees and may explain the heavy demand for shoulder and elbow experience. These findings are important for practice managers in designing equitable pay structures and the recruitment and retention of upper extremity surgeons.
References
- Eltorai AEM, Durand WM, Haglin JM, Rubin LE, Weiss AC, Daniels AH. Trends in Medicare reimbursement for orthopedic procedures: 2000 to 2016. Orthopedics. 2018;41(2):95–102. doi:10.3928/01477447-20180226-04 [CrossRef] PMID:29494748
- Kakar S, Bakri K, Shin AY. Survey of hand surgeons regarding their perceived needs for an expanded upper extremity fellowship. J Hand Surg Am. 2012;37(11):2374–2380. doi:10.1016/j.jhsa.2012.08.013 [CrossRef] PMID:23101535
- Brunworth LS, Chintalapani SR, Gray RR, Cardoso R, Owens PW. Resident selection of Hand Surgery Fellowships: a survey of the 2011, 2012, and 2013 Hand Fellowship graduates. Hand (N Y). 2013;8(2):164–171. doi:10.1007/s11552-013-9504-y [CrossRef] PMID:24426913
- Jupiter J. Hand surgery fellowships: time for reconsideration?Tech Hand Up Extrem Surg. 2011;15(4):197. doi:10.1097/BTH.0b013e31823d23eb [CrossRef] PMID:22105629
- Procedure Summary Tables: Medicare National HCPCS Aggregate table, CY 2015. cms.gov. Accessed August 2, 2018. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/Physician-and-Other-Supplier2015.html
- CY 2018 PFS Final Rule Addenda. cmc.gov. Accessed August 2, 2018. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1676-F.html
- Gaskill T, Cook C, Nunley J, Mather RC. The financial impact of orthopaedic fellowship training. J Bone Joint Surg Am. 2009;91(7):1814–1821. doi:10.2106/JBJS.H.01139 [CrossRef] PMID:19571105
- Elkousy H, Gartsman GM, Edwards TB, Heaps B, Laughlin MS, Press CM. Financial impact of third-party reimbursement changes for CPT Code 29826: experience of a large group practice. J Bone Joint Surg Am. 2014;96(21):e183, 1–6. doi:10.2106/JBJS.M.01173 [CrossRef] PMID:25378516
- Sears ED, Larson BP, Chung KC. A national survey of program director opinions of core competencies and structure of hand surgery fellowship training. J Hand Surg Am. 2012;37(10):1971–1977.e7. doi:10.1016/j.jhsa.2012.06.034 [CrossRef] PMID:22939829
- NCCI Policy Manual for Medicare Services. cms.gov. Accessed August 12, 2019. https://www.cms.gov/Medicare/Coding/National-CorrectCodInitEd/index.html
wRVUs/min Rates based on NSQIP Operative Time for 27 of the Most Common Shoulder/Elbow CPT Codes, According to Centers for Medicare and Medicaid Services.
| CPT Code | Procedure | wRVU | Median Operative Time (min) (NSQIP) | No. CMS Procedures | |
|---|---|---|---|---|---|
| 23474 | TSA revision (humerus and glenoid) | 0.24 | 27.21 | 112 | 3401 |
| 24358 | Tenotomy, elbow, debridement (open) | 0.24 | 6.66 | 28 | 1153 |
| 29807 | SA: SLAP repair | 0.23 | 14.67 | 65 | 4290 |
| 23420 | Rotator cuff reconstruction, complete | 0.23 | 13.54 | 60 | 6740 |
| 23473 | TSA revision (humerus or glenoid) | 0.23 | 25 | 111 | 1778 |
| 29806 | SA: capsulorrhaphy | 0.22 | 15.14 | 70 | 2144 |
| 23472 | TSA | 0.21 | 22.13 | 105 | 68977 |
| 29827 | SA: rotator cuff repair | 0.20 | 15.59 | 77 | 114023 |
| 29828 | SA: biceps tenodesis | 0.20 | 13.16 | 65 | 23551 |
| 23412 | Rotator cuff repair, chronic (open) | 0.20 | 11.93 | 59 | 28734 |
| 29822 | SA: debridement, limited | 0.20 | 7.6 | 38 | 26064 |
| 29825 | SA: adhesion lysis with or without manipulation | 0.20 | 7.79 | 39 | 5077 |
| 23120 | Claviculectomy, partial | 0.20 | 7.39 | 37 | 14103 |
| 29823 | SA: debridement, extensive | 0.20 | 8.36 | 42 | 45835 |
| 23405 | Tenotomy, shoulder area (single) | 0.19 | 8.54 | 44 | 3900 |
| 23410 | Rotator cuff repair, acute (open) | 0.18 | 11.39 | 62 | 7047 |
| 23470 | Hemiarthroplasty | 0.18 | 17.89 | 99 | 4648 |
| 23130 | Acromioplasty w/wo CA ligament release | 0.18 | 7.77 | 43 | 3651 |
| 29821 | SA: synovectomy, complete | 0.17 | 7.89 | 46 | 3238 |
| 23020 | Capsular contracture release | 0.17 | 9.36 | 55 | 1982 |
| 23440 | Biceps tendon resection | 0.16 | 10.64 | 65 | 2691 |
| 29824 | SA: distal claviculectomy | 0.16 | 8.98 | 55 | 72833 |
| 29819 | SA: foreign body removal | 0.16 | 7.79 | 50 | 2285 |
| 23430 | Tenodesis, biceps | 0.15 | 10.17 | 67 | 25312 |
| 24342 | Biceps/triceps tendon rupture reinsertion | 0.15 | 10.86 | 72 | 2914 |
| 24363 | Total elbow arthroplasty | 0.15 | 22 | 146 | 1025 |
| 24343 | Lateral collateral ligament repair | 0.13 | 9.16 | 68 | 1029 |
wRVUs/min Rates Based on NSQIP Operative Time for 53 of the Most Common Hosptial-based Hand Procedures, According to Centers for Medicare and Medicaid Services.
| CPT Code | Procedure |
wRVU | Median Operative Time (min) (NSQIP) | No. CMS Procedures | |
|---|---|---|---|---|---|
| 25115 | Excision of bursa, flexor tendons, wrist | 0.37 | 10.09 | 27 | 4,802 |
| 24359 | Epicondyle debridement w/tendon repair | 0.26 | 8.98 | 35 | 1,749 |
| 25295 | Tenolysis, forearm/wrist | 0.20 | 6.72 | 33 | 2,295 |
| 26952 | Amp thumb/finger phalanx, w/local flap | 0.20 | 6.48 | 32 | 2,086 |
| 26951 | Amp thumb/finger phalanx, direct closure | 0.20 | 6.04 | 30 | 8,011 |
| 26727 | Phalanx percutaneous pinning | 0.20 | 5.42 | 27 | 2,896 |
| 25116 | Excision of bursa, wrist/forearm | 0.20 | 7.56 | 38 | 1,391 |
| 25609 | Distal radius IA (>3 fragments) ORIF | 0.19 | 14.38 | 75 | 21,878 |
| 25076 | Excision tumor, forearm/wrist | 0.19 | 6.74 | 36 | 1,087 |
| 25000 | Incision extensor tendon (deQuervain’s) | 0.19 | 3.55 | 19 | 12,383 |
| 26746 | MCPJ or IPJ ORIF | 0.17 | 9.80 | 57 | 1,207 |
| 15736 | Muscle flap, upper extremity | 0.17 | 17.04 | 100 | 1,583 |
| 64702 | Neuroplasty, digital | 0.17 | 6.26 | 37 | 1,247 |
| 25020 | Decompression fasciotomy forearm/wrist | 0.17 | 6.06 | 36 | 1,408 |
| 25608 | Distal radius IA (2 fragments) ORIF | 0.17 | 11.07 | 67 | 10,229 |
| 25447 | Arthroplasty, interpostion, IC or CMC | 0.16 | 11.14 | 69 | 29,021 |
| 26910 | Ray amp | 0.16 | 7.79 | 50 | 1,409 |
| 25118 | Synovectomy, extensor, wrist | 0.15 | 4.51 | 30 | 2,627 |
| 26540 | Collateral ligament repair MCPJ or IPJ | 0.15 | 6.60 | 44 | 1,731 |
| 25607 | Distal radius EA ORIF | 0.15 | 9.56 | 64 | 13,066 |
| 26765 | Distal phalanx ORIF | 0.15 | 5.86 | 40 | 1,506 |
| 25320 | Carpal stabilization | 0.14 | 12.75 | 90 | 1,180 |
| 25545 | Ulna shaft ORIF | 0.14 | 7.94 | 58 | 1,802 |
| 26437 | Realignment of extensor tendon, hand | 0.13 | 5.99 | 45 | 2,447 |
| 25290 | Tenotomy, forearm/wrist | 0.13 | 5.43 | 41 | 2,994 |
| 26440 | Tenolysis, flexor tendon, palm/finger | 0.13 | 5.16 | 39 | 2,988 |
| 24341 | Tendon/muscle repair upper arm/elbow | 0.13 | 9.49 | 73 | 1,219 |
| 26615 | Metacarpal ORIF | 0.13 | 7.07 | 55 | 2,548 |
| 23030 | Abscess drainage shoulder | 0.13 | 3.47 | 27 | 1,139 |
| 26418 | Extensor tendon finger repair | 0.13 | 4.47 | 35 | 2,804 |
| 25111 | Excision of ganglion, wrist | 0.13 | 3.53 | 28 | 8,498 |
| 26735 | Phalanx shaft (proximal or middle) ORIF | 0.12 | 7.42 | 60 | 1,932 |
| 29846 | Arthroscopy, wrist, TFCC repair/excision | 0.12 | 6.89 | 56 | 2,181 |
| 24105 | Excision of olecranon bursa | 0.12 | 3.78 | 31 | 5,708 |
| 26356 | Repair flexor tendon (Zone 2) | 0.12 | 9.56 | 80 | 1,454 |
| 26410 | Extensor tendon hand repair | 0.12 | 4.77 | 40 | 1,629 |
| 26445 | Tenolysis extensor tendon, hand or finger | 0.12 | 4.45 | 38 | 2,038 |
| 24685 | Proximal ulna ORIF | 0.12 | 8.37 | 72 | 9,065 |
| 25575 | Radial and ulnar shaft ORIF | 0.12 | 12.29 | 106 | 1,336 |
| 24305 | Tendon lengthening, upper arm/elbow | 0.12 | 7.62 | 66 | 1,079 |
| 25260 | Tendon/muscle repair forearm/wrist | 0.11 | 8.04 | 71 | 1,153 |
| 25210 | Carpectomy, single bone | 0.11 | 6.12 | 55 | 3,093 |
| 26525 | Capsulectomy/capsulotomy IPJ | 0.11 | 5.50 | 50 | 2,044 |
| 26593 | Release, intrinsic muscles | 0.11 | 5.50 | 50 | 1,234 |
| 25280 | Lengthening/shortening tendon, forearm/wrist | 0.11 | 7.39 | 68 | 1,678 |
| 24666 | Radial head or neck ORIF | 0.11 | 9.86 | 92 | 1,236 |
| 26480 | Tendon transfer, CMC area or dorsal hand | 0.11 | 6.90 | 65 | 13,601 |
| 25215 | Proximal row carpectomy | 0.10 | 8.14 | 80 | 1,751 |
| 25310 | Tendon transplant/transfer, forearm/wrist | 0.10 | 8.08 | 82 | 11,830 |
| 26520 | Capsulectomy/capsulotomy MCPJ | 0.09 | 5.47 | 59 | 1,033 |
| 26531 | Arthroplasty MCPJ | 0.09 | 8.13 | 94 | 2,838 |
| 26536 | Arthroplasty IPJ | 0.09 | 6.56 | 76 | 1,763 |
| 25240 | Excision distal ulna (Darrach) | 0.08 | 5.31 | 66 | 1,655 |







{kind=link}