1. Introduction
]. The West Midlands has the fourth highest national rate of crime involving a knife or sharp instrument (111 per 100,000 population) [
]. Although knives and sharp objects account for the greatest proportion (39–45%) of homicides in the UK, the true burden of injury is more obscure []. The rise in knife crime is multifactorial. Contributory factors are thought to include income inequality and deprivation, school exclusion, adverse childhood environments and changes in the illicit drug trade [,
]. Police data demonstrate a national upward trend with all forms of violent crime; knife injuries account for only 4% of violence with injury but are associated with significantly higher mortality [
,
]. UK in-hospital mortality from knife injuries ranges between 0·5–8%, with deaths most commonly attributable to penetrating cardiac injuries [
,
,
,
]. Crucially, the incidence of knife crime appears to be rising despite considerable efforts at injury prevention.
]. In the UK, studies pertaining to knife injuries have largely been based in inner city London and the extent to which these findings are generalisable in other large urban areas, such as the Midlands and North of England, is unclear [
,
,
]. Studies indicate that assaults involving knives typically affect young men living in deprived, urban areas [
,
,
]. A public health approach to knife crime has been advocated on the basis that there are identifiable demographic and social risk factors, which may be amenable to intervention [
]. Government has proposed the imposition of Knife Crime Prevention Orders, involving a supervised programme of preventive rather than punitive measures [
]. This will include some prohibitions, such as a curfew, geographical and restriction of association, as well as positive elements such as educational courses, life skills programmes and targeted interventions [
,
]. There remains an urgent need to identify opportunities for targeted injury prevention and law enforcement strategies as part of a multi-agency effort to reduce knife injuries.
,
]. Indirect costs are much greater, including loss of psychological and social function to the individual, diminished community cohesion and, loss of economic productivity. A better understanding of knife-related injuries and the patients affected could facilitate targeted injury prevention strategies and aid resource planning within trauma systems of care. This study aimed to collate the epidemiological characteristics of knife-related injuries in order to further our understanding of knife crime victims. A secondary aim was to quantify the burden of knife injuries on Major Trauma Centre (MTC) resources.
2. Methods
]. Patients admitted following accidental or self-inflicted knife wounds were excluded. The setting is an urban MTC in Birmingham, UK, representing the highest tier of trauma care for all patients aged 16 years and above, within a regional trauma network. The centre receives patients living within its locality, as well as those who trigger the pre-hospital Major Trauma Triage Tool across a region encompassing a population of 2·44 million []. Those aged under 16 years are served by a separate paediatric regional MTC.
Patients were identified using three sources. The TARN database includes consecutive patients who attend hospital after sustaining injury who meet any of the following criteria: hospital length of stay greater than 72 h, admission to intensive care or in-hospital mortality. After meeting inclusion criteria, a hospital-based TARN audit co-ordinator will record prospectively collected variables into a standardised, web-based case record form including demographic, injury-related and outcome parameters. For these TARN-eligible patients, injury descriptions are coded centrally by TARN using the Abbreviated Injury Score (determined using manual AIS2005, Updated 2008), allowing calculation of Injury Severity Score (ISS). Additionally, the hospital’s blood bank maintains a prospective log of all massive transfusion protocol (MTP) activations; this log was perused to identify any trauma patients presenting within the three-year period, followed by screening of their medical records for eligibility. Furthermore, patients who attended the ED or the hospital with the discharge code “knife/sharp instrument” were identified retrospectively via the Hospital Informatics system and medical records were screened for eligibility.
].
]. As a registered hospital audit, no further ethical approval was required.
2.1. Data analyses
Data were collected using Microsoft Excel V·15·3 (Microsoft, California, USA) and analysed using R v3·6·1 software (R Core Team, Auckland, New Zealand, 2000). Continuous data are presented as medians and interquartile ranges (IQR) and categorical data are presented as frequencies (n) and percentages. Risk ratios and associated 95% confidence intervals and p-values were obtained using unadjusted log-binomial regression models, assessing the likelihood of sustaining injury in a domestic setting for female compared with male patients. The relationship between body region and weapon type and associated 95% confidence intervals was assessed using unadjusted log-linear multinomial regression models. The p-value for the relationship between body region and weapon type was obtained through a Monte Carlo simulation of Fisher’s exact test due to small cell frequencies. The relationships between weapon type and ISS and associated 95% confidence intervals and p-values were assessed using unadjusted linear regression models.
2.2 Role of funding
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
2.3 Data sharing statement
2.4 Patient consent
Not required.
2.5 Ethics approval
Not required, project registered with the Hospital Audit Department.
4. Discussion
]. TARN captured less than 50% of all patients admitted with knife injuries resulting from interpersonal violence. Knife injuries amongst women most commonly occurred within a domestic setting (65%), highlighting the problem of intimate partner violence. Injuries were attributable to machete use in 13·9% of patients. Our study also demonstrates a significant degree of violence recidivism, with nearly one in 5 patients presenting to our centre previously or subsequently with violence-related injuries during the observed period.
]. The true degree of recidivism may be higher than that demonstrated in our single-centre study. This finding of significant violence recidivism highlights an opportunity for secondary prevention and identifies the secondary care setting for delivery. The government-endorsed youth violence charity, RedThread has partnered with six NHS Hospital Trusts, most recently our own [
]. Following referral by a doctor or nurse, a RedThread youth worker builds rapport with the young victim of violence during their vulnerable period in the ED, at which point they may be receptive to engagement [
]. This is followed by efforts to enhance social factors that are deemed protective against violence, such as identifying avenues into education and employment, as well as signposting services such as housing and substance abuse programmes. Multi-agency collaboration between healthcare, local government and law enforcement has proved effective in Cardiff, Wales, where evidence has shown that the routine sharing of anonymised ED patient data with law enforcement to inform policing strategies has been associated with reductions in violent crime [
,
]. The community-focussed Cure Violence initiative has demonstrated similar results across several US cities [
]. As a minimum requirement, the General Medical Council specifies that clinicians have a statutory duty to report all knife injuries to the police [
]. Further research is required to determine whether the newly proposed Knife Crime Prevention Orders, issued by law enforcement alongside criminal conviction, are effective in reducing knife injuries [
].
]. Weapon description was unrecorded in 36·3% of patients and these patients were found to have a higher Injury Severity Score than those in whom precise causative weapon was recorded. Possible explanations for this finding are that patients with more severe injuries were less able to provide a detailed history of events, or that clinicians did not pursue or record weapon details when dealing with more severely injured patients. Whilst folding blades of three inches or less are currently legal to possess, they accounted for 40% of head and neck injuries in the study population, imposing major additional demands on healthcare resources; further studies to measure their involvement in violent crime in other regions are required and a review of their legal status is recommended. In August 2019, the Offensive Weapons Act 2019 specifically recognises the doubled-edged “zombie” and “cyclone” knives as offensive weapons, however no mention is made of machetes, which may be easily distinguished by their size [
,
]. The authors recommend that law enforcement agencies develop strategies to limit the availability of machetes and to view the possession of machetes in the UK as a serious crime, as it is likely that these have been purposefully acquired for use as weapons.
,
]. Of particular concern was the relatively high proportion of pregnant women sustaining stab wounds. Clinicians caring for female patients with knife injuries should routinely enquire about the identity of the perpetrator, particularly in those who present during pregnancy, and ensure that the necessary referral to law enforcement agencies and domestic abuse services is offered.
]. In order to objectively report prevalence and trends in violent injuries and, crucially, to measure the impact of any preventative strategies, the development of a regional or national registry including all knife injuries is urgently warranted.
,
]. Multiple specialists are often involved in the care of knife-injured patients, with favourable in-hospital mortality figures suggesting that care is well co-ordinated in the context of our regional major trauma network. The majority of deaths in our cohort were attributable to penetrating chest injuries, consistent with previous studies [
,
]. Thoracic trauma is common, occurring in 18% of patients, and often severe. For policy makers, this finding should provide impetus for co-locating cardiothoracic surgical services within MTCs. Whilst our in-hospital mortality is low, homicide data suggest that there have been almost four times the number of knife-related deaths within our region during our study period [
]. Further research is needed to determine the current injury pattern in those who die before reaching hospital, in order to elucidate the means by which these deaths may be prevented.
,
]. These findings reinforce the need for senior ED clinicians and surgeons to be readily available out of hours and during the summer months to tend to these patients, who have a high likelihood of requiring operative intervention (65%), as demonstrated in this study.
]. Intoxication with heroin was recorded in 4·7% of patients and cocaine in 1·7%. Whilst overall drug use appeared relatively unchanged during the period in which knife-related crime has increased, it is thought that changes in the drugs market, such as extension of heroin and cocaine distribution outside of urban areas into ‘county lines’ by drug-dealing gangs, have contributed to the increase in serious violence [,
]. Knowledge of drug and alcohol intoxication is clinically relevant as this may impact upon patients’ neurological status and physiology, as well as their ability to give consent, with implications for anaesthesia/analgesia and the need for detoxification.
]. Challenges in the way that data are collected, both within healthcare and externally, make identification of the true direct and indirect costs associated with knife injuries difficult.
,
,
]. This study represents the more severe end of the knife injury spectrum by virtue of its major trauma centre setting. The findings may be more generalizable to urban centres in the Midlands and North of England as compared with previous London-based studies, as these cities share demographic similarities and have all experienced a sudden increase in knife crime in the last 5 years [
]. An inherent weakness of this study include its retrospective nature and that the study was based in an adult MTC. With growing public concern regarding the involvement of minors in knife-related incidences, as highlighted in the media and national hospital admission reports, future studies should include specialist children’s hospitals [,
,].
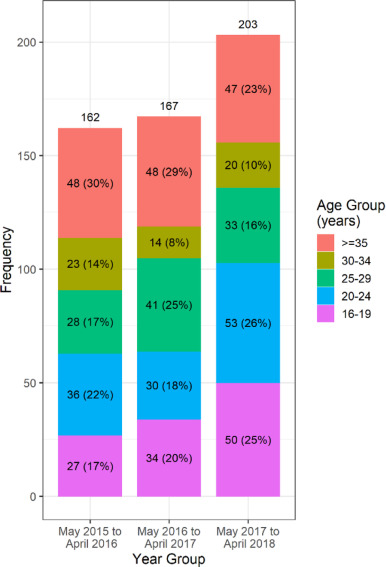
Knife-related injuries consume a large amount of secondary care resources, constituting 12·9% of the trauma team workload at our MTC. A thorough understanding of patient and injury characteristics will be beneficial in future resource planning. Our study has illustrated that knife injuries predominantly affect young men under the age of 25 years and that the overall increase in incidence is accounted for by this demographic. Reliance on the national major trauma database significantly under-represents the true burden of knife injuries. Our novel findings of a significant degree of violence recidivism and machete use have several potential implications for targeted violence-reduction and law enforcement strategies. An important minority of knife-injured patients are women injured by intimate partners. There is an urgent requirement to generate a national collaborative database to inform multi-agency strategies in the prevention and treatment of violent penetrating injury. Healthcare must continue to play an important role as part of a multi-agency approach to better understand and address the important public health issue of knife crime.
4.1. Transparency statement
NM guarantees that the manuscript is an honest, accurate, and transparent account of the study being reported. No important aspects of the study have been omitted.







{kind=link}