Abstract
Background
Multiple sclerosis (MS) is a leading cause of disability among young adults and effects considerable social and economic burdens. Data of MS incidence in China at the national level is lacking. We conducted the first nationwide hospital-based study to estimate the incidence and hospitalization burden of MS in China.
Methods
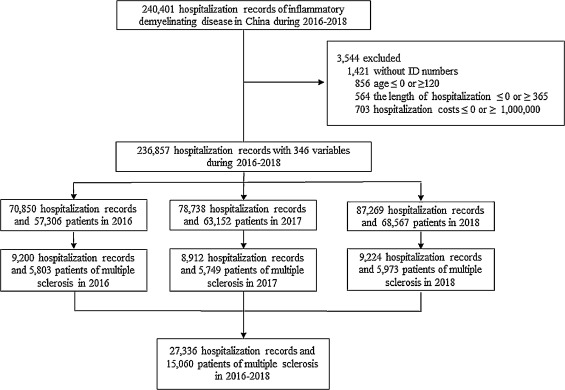
This study is based on an administrative database of the National Hospital Quality Monitoring System, which covers all 1665 tertiary hospitals in mainland China. The “Medical Record Homepage” of all patients, including 346 variables including demographic characteristics, diagnoses, procedures, and expenses etc., were uniformly collected across each tertiary hospital via standard protocol. MS was defined by the 2010 International Panel criteria for MS and was identified by ICD-10 code (G35•0).
Findings
We identified 27,336 hospital admissions for 15,060 MS patients from 2016 to 2018; amongst these patients, 9,879 were newly diagnosed. The age- and sex-adjusted incidence per 100,000 person-years is 0•235 (95% confidence interval [CI] 0•230–0•240), with 0•055 (0•050–0•060) in children and 0•288 (0•282–0•294) in adults, respectively. The female to male ratio is 2•02; the peak disease onset is age of 40–49 years. Residents in high-latitude and high-altitude areas are more likely to develop MS (F = 8•99; p < 0•001). Prevalent comorbidities include hypertension (18•8%), diabetes (7•2%), stroke (14•7%), depression or anxiety (3•7%), and autoimmune disease (2•3%). Through 2016–2018, 104 adults and 2 children died, with a hospital mortality rate of 9•9 per 1,000 person-years.
Interpretation
For the first time, we obtain the national incidence of MS as 0.055 in children and 0.288 in adults per 100,000 in China. The geographical distribution of MS incidence presented a north-south latitude gradient and a west-east altitude gradient.
Funding
National Science Foundation of China (81801199, 91642205, and 81830038); Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing.
1. Introduction
]. Nearly 1 million MS patients were confirmed with associated costs of over $24 billion annually in the United States [
]. In 2020, Public Health England revealed about 4950 people are diagnosed with MS each year in United Kingdom [
].
]. However, the worldwide prevalence of MS varies substantially between the continents due to geographical and environmental characteristics. The landmark epidemiological studies from Kurtzke and colleagues assumed the frequency of MS was related to latitude with three; high, moderate, and low “zones” [
]. The highest age-standardized MS prevalence was 164•6 in high-income North America, 127 in western Europe, and 91•1 in Australasia, and the lowest were 3•3 in eastern sub-Saharan Africa, 2•8 in central sub-Saharan African, and in Oceania, 2 per 100,000 persons [
].
]. The nationwide Japanese survey conducted in 2004 estimated the prevalence of MS at 7•7 per 100,000 [
]. The age-standardized prevalence per 100,000 persons was 3•23 in Korea [
] and 2•73 in Malaysia [
]. However, in China, which accounts for 21•6% of Asia’s land area and 18•8% of the world’s population, the epidemiological data on MS is absent or extremely sparse. The two epidemiological studies available are regionally narrow; one showed the MS prevalence rate of 1•39 per 100,000 in Shanghai, the other in Shandong Province estimated an incidence rate of 0•20 per 100,000 for females and 0•12 for males [
,
].
In this study, we estimate the incidence of MS in mainland China between 2016 and 2018 using a nationwide administrative database of Hospital Quality Monitoring System (HQMS), which is maintained by the National Health Commission (NHC).
4. Discussion
], geographical distribution of MS risk can be generally distributed in three zones, with North American and northern European countries considered as a high-risk prevalence zone. Asia has been among the low-risk areas, although incidence has been recently increasing [
]. According to the 2013 Atlas of MS launched by the Multiple Sclerosis International Federation, MS prevalence is highest in Middle East and lowest in East Asia [
]. The incidence of MS in Iran reached 6•7/100,000, similar to continental Europe [
]. However, the incidence of MS in East Asian countries is at comparable levels range from 0•2 to 0•8 per 100,000 persons. In the present study, the incidence of MS in Inner Mongolia and Shanxi Province, which are in the same latitude zone as Japan and South Korea, were 0•33 and 0•54 /100,000. The age-standardized incidence of MS was 0•50 per 100,000 in Korea [
], In Japan, the incidence is on the rise from 0•04 in 1980s to 0•78 /100,000 in 2004 [
]. Malaysia, with 23.4% ethnic Chinese, observed a crude annual incidence of 0•55 per 100,000 [
]. In addition to estimating at the national incidence, a map of MS incidence in 31 provinces and municipalities was compiled. We found that the incidence of MS in Shandong Province is 0•29/100,000 for female and 0•12 for male, which is broadly consistent with a hospital-based study on MS incidence in Shandong Province in 2013 [
].
] a strong latitude gradient was detected for the prevalence of MS, with a 1•03 times increase in prevalence per latitude degree [
]. Moreover, residents living at higher latitude are associated with a younger age of MS onset [
]. Differential exposure to sunlight has been posited as an environmental cause accounting for the positive association between MS incidence and latitude, as ultraviolet (UV) light stimulates the production of vitamin D in the body [
,
]. The link between vitamin D insufficiency and increased risk of MS is well identified [
]. Although higher altitudes generally correspond to increased UV radiation exposure, vitamin D levels do not necessarily increase. A study to compare serum vitamin D levels of plateau Tibetan peoples with Han peoples in Sichuan basin, showed lower serum 25-hydroxy vitamin D in highland Tibetan [
]. Temperature and UV are both factors that stimulate vitamin D production. The climate in the plateau is marked by low temperature. The exposure of the skin is less during outdoor activities in the highland area [
]. Temperature, exposure, diet, and supplements are all confounding factors which obscure vitamin D3s role in manifestation of MS incidence.
]. The incidence of NMOSD and MS in Korea was 0•73 and 0•50 per 100,000 persons, respectively [
]. The ratio of NMOSD to MS among the Chinese Malaysians was 2•0:1•0 [
]. A female predominance was observed in the incidence of both NMOSD and MS, but the difference was more pronounced in NMOSD. In our study, the female to male sex ratio of MS and NMOSD was 2•02 and 4•71. The sex ratio of MS varied among different studies with an estimated 3•4:1 in East Asia, following 2•1 in Japan, 1•6 in Korea, 3•2 in Hong Kong, and 3•4 in Taiwan [
]. The female propensity for NMOSD was evident in the Chinese Malaysians rather than for MS by a female to male ratio at 5:1 versus 12:1 in Malaysia [
].
]. This is likely attributable to the 2010 McDonald diagnostic criteria for MS, which facilitates earlier diagnosis. Adults developed MS at a later age in China. this could be related to our study method which defines incidence based on new diagnoses rather than time of symptom manifestation, due to the restriction in HQMS information logging.
]. Few well-designed population-based studies have assessed the incidence or prevalence of autoimmune diseases, cancers, and stroke among patients with MS. Our data report these comorbidities in MS patients as: autoimmune diseases (2•3%), cancers (1•3%), and stroke (14•7%). Depression is the most common associated mental disorder in patients with MS on hospital-based clinics survey [
]. A population-based study evaluated the prevalence of comorbidity at the time of diagnosis in 16,803 Canadian MS patients, wherein a large proportion of patients with MS developed major depression (19•1%) and anxiety (11•1%) [
]. However, the incidence of depression was a relatively low 3•7% in our study. This may be attributed to HQMS only collecting inpatient information and the majority of patients with depression or anxiety are followed up in the clinic. We noticed a high frequency of stroke in MS, in part due to the very high prevalence of stroke in China (1114.8 to 2370/100,000 in China vs 434.86 to 502.32/100,000 the rest of the world) [
,
].
]. Mortality rates due to infectious diseases and diseases of the respiratory system were higher within the MS population [
].
Our study has several limitations. First, we did not have access to outpatient records. Certain patients with mild symptoms may be diagnosed with clinically isolated syndrome and followed by outpatient visits. The actual incidence may be higher than our current data. Second, results of oligoclonal IgG bands and MRI findings were not collected in this study. Third, we were unable to calculate the prevalence of MS in this study. Prevalence is the product of the incidence rate and the average duration of a condition. The prevalence of MS in China can be well estimated when HQMS contains decades of data in the future.
For the first time, our study captures the incidence for multiple sclerosis across all age groups in almost all Chinese patients. The unique administrative national database enhances the accuracy and rigor of these estimates. The geographical distribution of MS incidence not only correlates to the north-south latitude gradient but also to west-east altitude gradient. Our study fills in the blank of epidemiologic data for approximately 1.4 billion Chinese and enriches the global outlook for this disease. The reported disease burden calls for ramping up regional and global efforts to care for MS patients and investment in research for this devastating and pervasive disease.
Contributors
F.-D.S. and Y.W. conceived and designed this study; F.-D.S., D.-C. T., Z. L., C. Z., M.Y. and X. Y. acquired and analyzed the data; and F.-D.S., D.-C.T., C. Z., drafted the manuscript and prepared the figures; H. G. was involved in statistics analysis; F-D.S. obtained funding; F.-D. S. made critical revisions of the manuscript and important intellectual contributions. All authors reviewed the manuscript.
Data sharing
The study protocol, statistical analysis plan, and deidentified data that underlie the results of this article will be available for investigators after approval by the Institutional Review Board of China National Clinical Research Center for Neurological Diseases (Beijing, China). Please email the corresponding author for more information.
Acknowledgements
We thank colleagues from National Center for Quality Control of Neurological Diseases for technical and logistic support; Samuel X. Shi for English editing; Yingyu Jiang for statistical analysis.
Editor note: The Lancet Group takes a neutral position with respect to territorial claims in published maps and institutional affiliations.







{kind=link}