There are concerns that the response to the COVID-19 pandemic in the UK might have worsened physical and mental health, and reduced use of health services. However, the scale of the problem is unquantified, impeding development of effective mitigations. We aimed to ascertain what has happened to general practice contacts for acute physical and mental health outcomes during the pandemic.
Methods
Using de-identified electronic health records from the Clinical Research Practice Datalink (CPRD) Aurum (covering 13% of the UK population), between 2017 and 2020, we calculated weekly primary care contacts for selected acute physical and mental health conditions: anxiety, depression, self-harm (fatal and non-fatal), severe mental illness, eating disorder, obsessive-compulsive disorder, acute alcohol-related events, asthma exacerbation, chronic obstructive pulmonary disease exacerbation, acute cardiovascular events (cerebrovascular accident, heart failure, myocardial infarction, transient ischaemic attacks, unstable angina, and venous thromboembolism), and diabetic emergency. Primary care contacts included remote and face-to-face consultations, diagnoses from hospital discharge letters, and secondary care referrals, and conditions were identified through primary care records for diagnoses, symptoms, and prescribing. Our overall study population included individuals aged 11 years or older who had at least 1 year of registration with practices contributing to CPRD Aurum in the specified period, but denominator populations varied depending on the condition being analysed. We used an interrupted time-series analysis to formally quantify changes in conditions after the introduction of population-wide restrictions (defined as March 29, 2020) compared with the period before their introduction (defined as Jan 1, 2017 to March 7, 2020), with data excluded for an adjustment-to-restrictions period (March 8–28).
Findings
The overall population included 9 863 903 individuals on Jan 1, 2017, and increased to 10 226 939 by Jan 1, 2020. Primary care contacts for almost all conditions dropped considerably after the introduction of population-wide restrictions. The largest reductions were observed for contacts for diabetic emergencies (odds ratio 0·35 [95% CI 0·25–0·50]), depression (0·53 [0·52–0·53]), and self-harm (0·56 [0·54–0·58]). In the interrupted time-series analysis, with the exception of acute alcohol-related events (0·98 [0·89–1·10]), there was evidence of a reduction in contacts for all conditions (anxiety 0·67 [0·66–0·67], eating disorders 0·62 [0·59–0·66], obsessive-compulsive disorder [0·69 [0·64–0·74]], self-harm 0·56 [0·54–0·58], severe mental illness 0·80 [0·78–0·83], stroke 0·59 [0·56–0·62], transient ischaemic attack 0·63 [0·58–0·67], heart failure 0·62 [0·60–0·64], myocardial infarction 0·72 [0·68–0·77], unstable angina 0·72 [0·60–0·87], venous thromboembolism 0·94 [0·90–0·99], and asthma exacerbation 0·88 [0·86–0·90]). By July, 2020, except for unstable angina and acute alcohol-related events, contacts for all conditions had not recovered to pre-lockdown levels.
Interpretation
There were substantial reductions in primary care contacts for acute physical and mental conditions following the introduction of restrictions, with limited recovery by July, 2020. Further research is needed to ascertain whether these reductions reflect changes in disease frequency or missed opportunities for care. Maintaining health-care access should be a key priority in future public health planning, including further restrictions. The conditions we studied are sufficiently severe that any unmet need will have substantial ramifications for the people with the conditions as well as health-care provision.
Funding
Wellcome Trust Senior Fellowship, Health Data Research UK.
Results
The overall denominator population included 9 863 903 individuals on Jan 1, 2017, and numbers remained relatively stable throughout the study (table 2). The characteristics of condition-specific study populations are shown in the appendix (pp 4–8).
Table 2General denominator population defined in the first week of each year from 2017 to 2020
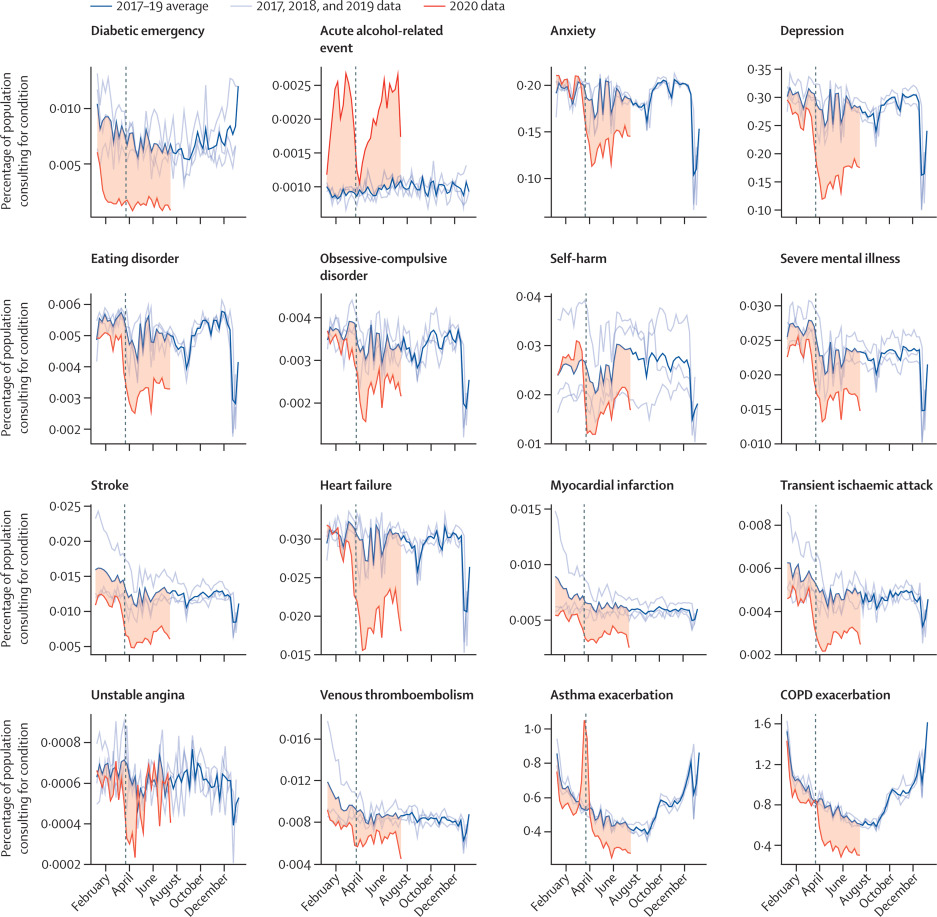
Figure 1 shows the percentage of a given study population with primary care contacts for each condition in 2020 and a 3-year historical average for the corresponding week. Across the majority of conditions, we observed rapid and sustained decreases in GP contacts between March and July, 2020, compared with pre-lockdown periods. Despite gradual increases in contacts as a percentage of denominator population following restrictions, levels remained below the 3-year average for all conditions except acute alcohol-related events (which were higher than the historical average in 2020) and unstable angina. During March, 2020, we observed pronounced increases in contacts related to asthma exacerbations. Patterns were broadly consistent when stratified by age (figure 2), sex, region, and ethnicity (appendix pp 9–11).
Figure 1Proportions of each study population with contacts for each condition in 2017–19 and 2020
Percentage of eligible population with contacts for each health condition studied in 2020 compared with the historical (2017–19) average for that week. Shaded regions show the difference between the 2020 data and the historical average. Vertical dashed lines indicate the introduction of lockdown restrictions in the UK on March 23, 2020. Tick marks on the x-axis represent the first day of the specified month. COPD=chronic obstructive pulmonary disease.
Figure 2Percentage of each denominator population with general practitioner contacts for the study conditions throughout 2020, by age group
Coloured lines represent weekly percentages of the eligible population with primary care contacts for the condition of interest in 2020; eligible populations differed by condition (table 1). Boxplots represent the historical average (median and IQR) percentage of the study population with general practitioner contacts for the condition of interest. Vertical dashed lines indicate the introduction of lockdown restrictions in the UK on March 23, 2020. Tick marks on the x-axis represent the first day of the specified month. Note that cell counts with fewer than five contacts in 1 week in 2020 have been suppressed. COPD=chronic obstructive pulmonary disease.
There was evidence that contacts for all studied conditions, except acute alcohol-related events, were lower after restrictions were announced compared with pre-restriction levels (figure 3A). The largest relative reductions in contact behaviour following restriction introduction were observed for diabetic emergencies (OR 0·35 [95% CI 0·25–0·50]), depression (0·53 [0·52–0·53]), and self-harm (0·56 [0·54–0·58]). With the exception of acute alcohol-related events (0·98 [0·89–1·10]), there was evidence of a reduction in contact behaviour for all conditions studied: anxiety 0·67 (0·66–0·67), eating disorders 0·62 (0·59–0·66), obsessive-compulsive disorder (0·69 [0·64–0·74]), self-harm 0·56 (0·54–0·58), severe mental illness 0·80 (0·78–0·83), stroke 0·59 (0·56–0·62), transient ischaemic attack 0·63 (0·58–0·67), heart failure 0·62 (0·60–0·64), myocardial infarction 0·72 (0·68–0·77), unstable angina 0·72 (0·60–0·87), venous thromboembolism 0·94 (0·90–0·99), and asthma exacerbation 0·88 (0·86–0·90; figure 3B; appendix p 17).
Figure 3Interrupted time-series analysis of changes in general practitioner contacts before and after the introduction of UK-wide restrictions
(A) Lines indicate the observed percentage of the denominator population with primary care contacts for each health condition in 2020. Shaded regions indicate the predicted percentage of contacts from the full interrupted time-series model (including data from 2017 onwards). Vertical lines show the adjustment-to-restrictions period from which data were excluded from the analysis (March 8–28, 2020). Tick marks on the x-axis represent the first day of the specified month. (B) 95% CIs of ORs for the estimated relative reduction in contacts as a percentage of the denominator population for each health condition immediately after the adjustment-to-restrictions period (March 29, 2020) compared with the pre-lockdown period (values closer to 0 represent a greater reduction in the estimated percentage of people with general practitioner contacts). (C) 95% CIs of ORs for the estimated effect of time (in weekly increments) since the introduction of restrictions (March 29, 2020)on contacts as a percentage of the denominator population for each condition (values >1 indicate an increasing percentage of population with contacts over time). Results for 2020 only are shown here (see appendix p 24 for full model fit to data from 2017, and appendix pp 17–18 for full relative reduction and recovery ORs and 95% CIs). COPD=chronic obstructive pulmonary disease. OR=odds ratio.
From March 29, 2020, we saw evidence of increasing contacts for most conditions over time. Acute alcohol-related events and unstable angina contacts appeared to recover faster (3–5% increase in odds of contact per week; figure 3C; appendix p 18) than, for example, mental health contacts, for which odds of contact increased by 1–2% per week despite a 20–47% drop following restrictions (figure 3B; appendix p 17). Sensitivity analyses using varying exclusion periods between pre-lockdown and with-restrictions periods provided broadly consistent results over a range of scenarios (appendix pp 17–25).
Table 3 shows the potential impact of reduced contacts on relevant populations. For some rare conditions, such as unstable angina and acute alcohol-related events, the absolute change in contacts was relatively small; however, other more common conditions had a larger absolute change in contacts. For example, compared with expected numbers of COPD exacerbation contacts per million people with COPD, we estimated that there were cumulatively 43 900 fewer contacts between March 29 and July 4; there were 3640 fewer contacts from April 26 to June 2 and 3230 fewer from June 28 to July 4, indicating a slow return to pre-lockdown contact levels but not complete recovery. Cumulatively between March 29 and July 4, we also estimated 14 100 fewer asthma exacerbation contacts for every million people with asthma, 12 800 fewer depression contacts per million people in the denominator population, and 6600 fewer anxiety contacts per million people in the denominator population.
Table 3Estimated reduction in number of primary care contacts
Data represent the estimated number of primary care contacts for acute physical and mental health conditions in a hypothetical non-COVID-19 year compared with the number of contacts estimated from our model for 2020 for two week-long periods: April 26–May 2 and June 28–July 4. Estimates of the number of contacts are in a hypothetical population of 1 million people, but the reference populations are condition specific (table 1). COPD=chronic obstructive pulmonary disease.
Discussion
Primary care contacts for key physical and mental health conditions dropped considerably after the introduction of population-wide restriction measures in March, 2020. By July, 2020, with the exception of unstable angina and acute alcohol-related contacts, primary care contacts for all conditions studied remained below pre-lockdown levels. We estimated that by July, 2020, per million people in the general population, there were very small (<10) drops in the cumulative number of contacts for myocardial infarction, unstable angina, and venous thromboembolism. However, we estimated large drops for anxiety, depression, and COPD contacts.
Our study is the first to explore the effect of lockdown measures on primary care contacts for specific acute physical and mental health conditions across the UK. A study of 47 primary care practices in Salford, a largely deprived urban area in northwest England that was badly affected by the pandemic, suggested that primary care consultations across four broad categories (common mental health problems, cardiovascular and cerebrovascular disease, type 2 diabetes, and cancer) had reduced by up to 50% by the end of May, 2020.
Diagnosis of physical and mental health conditions in primary care during the COVID-19 pandemic: a retrospective cohort study.
In contrast to the Salford study, our sample was nationally representative and focused on contacts for specific disease categories that we would expect to present to health-care providers. Our large sample size allowed us to investigate detailed diagnoses (for example, different types of cardiovascular disease and mental health conditions).
In September, 2020, GPs conducted more face-to-face appointments than any week since March, and more consultations overall than before the pandemic (40% were telephone appointments).
A study of 51 GP practices already offering remote consultations before the pandemic indicated a dip in overall consultations at the time of lockdown but, unlike our results for specific acute conditions, their post-lockdown overall consultation decrease was less extreme than that during the Christmas period of 2019.
How has NHS 111 shaped public demand for the NHS in England during the pandemic?.
The reduced diabetic emergency contacts we observed are consistent with the 49% reduction in new type 2 diabetes contacts (new prescriptions for metformin) in Salford. Although the Salford study highlighted missed new diagnoses, our study identifies missed contacts for acute deteriorations. Given that 90% of diabetes management is in primary care, the large relative reduction in the proportion of people with diabetes with diabetic emergency contacts is concerning.
Type 2 diabetes management in primary care: the role of retrospective, professional continuous glucose monitoring.
Recent evidence indicates a two-way interaction between diabetes and COVID-19, with a potentially causal association between COVID-19 infection and dysglycaemia, such that each condition exacerbates the other.
The impact of the COVID-19 pandemic on cardiology services.
Taken alongside findings of similar reductions in emergency department presentations and hospital admissions for cardiovascular outcomes in the UK, our findings highlight an area of major concern,
The 4C Initiative (Clinical Care for Cardiovascular disease in the COVID-19 pandemic)—monitoring the indirect impact of the coronavirus pandemic on services for cardiovascular diseases in the UK.
particularly as evidence from France indicates increased out-of-hospital cardiac arrest.
Indeed, it is possible that the more rapid recovery in unstable angina contacts (compared with other conditions included in our study) might reflect COVID-19-related cardiovascular disease. However, the number of unstable angina events recorded were small, so we are unable to draw any meaningful conclusions from these results.
Initial effects of the COVID-19 pandemic on pediatric asthma emergency department utilization.
There is no compelling evidence that individuals with asthma are at greater risk of severe COVID-19 outcomes, although there was uncertainty at the onset of the pandemic.
Viruses commonly trigger asthma exacerbations, so we might have expected to see more asthma contacts. Anecdotally, GPs reported increased prescription of asthma therapies around the lockdown period,
which could explain initial increased asthma contacts. Similar increases in COPD exacerbation contacts were not seen around the introduction of restrictions, despite our definition including prescriptions for oral corticosteroids. One explanation might be that, as COPD is a progressive respiratory condition, individuals with COPD might have repeat prescriptions, reducing the need (compared with people with asthma) to stockpile drugs in a crisis.
Surveys have reported increased anxiety, depression, and self-harm during the pandemic,
What happened to patients with obsessive compulsive disorder during the COVID-19 pandemic? A multicentre report from tertiary clinics in northern Italy.
COVID-19 and severe mental illness: impact on patients and its relation with their awareness about COVID-19.
However, we saw a sustained reduction in primary care contacts for anxiety, depression, and other mental health conditions consistent with other reports;
Diagnosis of physical and mental health conditions in primary care during the COVID-19 pandemic: a retrospective cohort study.
this finding is concerning because the majority of common mental disorders are managed in primary care. Similarly, the observed reduction in health-care contacts for people with severe mental illness is concerning because these individuals are likely to be at greater risk of poor outcomes from COVID-19 because of the high prevalence of risk factors for adverse outcomes in this group (eg, cardiovascular disease and deprivation).
Cardiovascular risk assessment in patients with a severe mental illness: a systematic review and meta-analysis.
Findings from surveys on alcohol consumption in lockdown have been mixed, with some reporting increased alcohol consumption in up to a third of people surveyed, while others had differing findings.
Institute of Alcohol Studies Alcohol consumption during the COVID-19 lockdown: summary of emerging evidence from the UK.
We saw primary care contacts for acute alcohol-related events increase before and after restrictions, which is troubling given the reduction in contacts for other conditions studied; however, we urge caution in drawing robust conclusions as numbers were small.
This study involved a rapid assessment of changes in primary care contacts following the introduction of UK population-wide restrictions up to July, 2020, in a large sample representative of the UK population. Historical data allowed us to compare observed patterns in 2020 with trends in the previous 3 years. We estimated relative and absolute changes in contact patterns, with a focus on easy to interpret measures.
Our study describes and quantifies the reduction in primary care contacts across a wide range of health conditions likely to be affected by COVID-19 to generate hypotheses. However, further research is needed to understand the specific drivers behind these changes (eg, individuals could have limited their in-person contact through fear of SARS-CoV-2 infection, or might have had difficulty accessing primary care services because of unavailability of appointments or lack of available technology or technological literacy for virtual consultations). It is important that we understand what happened to individuals who did not consult their GP—specifically, whether they were treated in secondary care or self-managed, and to what extent our findings can be explained by genuine changes in disease frequency.
Without hospital and mortality data, we are unable to investigate whether, for example, any reduction in GP contacts resulted in corresponding increases in hospital attendances or deaths. We focused on studying any record of our conditions of interest, so our results reflect all primary care contacts, including diagnoses recorded by general practice staff from hospital discharge letters. Consequently, a potential explanation for our findings is that individuals with some of the emergency conditions studied might have presented directly to hospital for their emergency non-COVID-19 condition, with delayed recording of hospital discharge diagnoses in primary care health records as a result of changes in administrative practices in response to the pandemic restrictions. Similarly, we were unable to account for individuals with chronic conditions being admitted directly to hospital with SARS-CoV-2 infection. However, hospital COVID-19 admissions are unlikely to have resulted in the magnitude of the abrupt change in primary care contacts that we saw: hospital admissions for COVID-19 were increasing in March, 2020, but government data suggest that on March 27 there were 7043 individuals in hospital with a confirmed COVID-19 diagnosis,
Public Health England Coronavirus (COVID-19) in the UK: healthcare in United Kingdom.
which would not account for the sudden and large decline in primary care contacts that we saw across most conditions studied.
Another potential explanation for our findings could be related to changes in how primary care contacts were documented following a rapid shift to remote consultations. However, we feel that the conditions we studied are sufficiently severe that it is unlikely that diagnoses would not have been recorded. To avoid problems arising from the timing of behavioural change associated with restrictions, our interrupted time-series analysis excluded a predefined intervention period when individuals’ behaviours were changing dynamically. We took a conservative approach and defined our intervention period between March 8 and March 28, 2020, assuming that some people would have modified their behaviour before the introduction of restrictions. Sensitivity analyses varying the start date showed consistent findings with those of the main analysis.
Detailed exploration of whether consultation behaviour varied in people considered clinically vulnerable and advised to shield
Impact of COVID-19 on accident and emergency attendances and emergency and planned hospital admissions in Scotland: an interrupted time-series analysis.
The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: a national, population-based, modelling study.
although one explanation could be genuine changes in disease frequency (which is unlikely, given consistent results across disease categories), it is more likely that our findings reflect missed opportunities for care. There are plausible mechanisms that might explain real reductions in frequency for some of our outcomes, such as better glycaemic control in diabetes because of more regular routines when staying home; less respiratory disease because of lower exposure to air pollution during lockdown,
Public Health England COVID-19: guidance on shielding and protecting people defined on medical grounds as extremely vulnerable.
and reduced alcohol consumption due to pub closures and reduced social contact. Conversely, there are plausible mechanisms that could explain genuine increased frequency of these conditions (eg, distress related to the pandemic affecting mental health and alcohol consumption, reduced exercise affecting cardiovascular health, changes in diet influencing glycaemic control). Additionally, for some of our outcomes, such as mental health conditions, some evidence indicates increased frequency.
What happened to patients with obsessive compulsive disorder during the COVID-19 pandemic? A multicentre report from tertiary clinics in northern Italy.
COVID-19 and severe mental illness: impact on patients and its relation with their awareness about COVID-19.
Increases in non-COVID-19-related excess mortality also make it more likely that our observed reduction in primary care contacts was due to behavioural changes rather than reduced disease frequency.
Neurological and neuropsychiatric complications of COVID-19 in 153 patients: a UK-wide surveillance study.
indicates that we might have expected more need for care for these conditions as a direct result of the pandemic.
Our results are likely to represent a large burden of unmet need, particularly in relation to COPD and mental health conditions. Health-care providers should prepare for increases in morbidity and mortality in the coming months and years. Further research should address whether reduced clinical contact has resulted in excess mortality, and whether we need to increase service provision for individuals with increased health-care needs resulting from delaying seeking access to care. Although numbers of unstable angina events were small, we note a more rapid return to pre-pandemic consultation rates compared with that of other study outcomes; this observation needs investigation as it could be a direct consequence of the pandemic. Future research should also investigate potential behavioural drivers of the changes in primary care contacts we observed (eg, reluctance to initiate health-care contact, difficulty in making primary care appointments, or concerns about using information technology for remote consultations), as well as the effect of multiple periods of lockdown restrictions being imposed and lifted, and should include similar international studies to investigate the global implications of the pandemic on non-COVID-19 illness. Finally, our findings highlight a need to ensure equitable access to primary care in future pandemic planning, particularly with the added burden on primary care of vaccine delivery. Countries such as Singapore, which had experienced severe acute respiratory syndrome, implemented control measures in primary care rapidly.
These lessons must be systematised and implemented.
In summary, this study showed substantial reductions in primary care contacts for various acute physical and mental health conditions. Our findings are likely to represent a considerable burden of unmet need, which might lead to substantial increases in subsequent mortality and morbidity.
All study authors were involved in the development of the study, contributed to the development of the code lists that defined the variables used in the study, and contributed to and approved the final manuscript. RM, JT, ADH, HC, PB, and AYSW were responsible for data management. RM, JT, ADH, and ARM were responsible for statistical analyses. KEM, RM, JT, ADH, and ARM wrote the first draft of the Article. All authors had access to all the data in the study, and all authors had final responsibility for the decision to submit for publication. HC, JT and RM accessed and verified the data.
RM reports personal fees from Amgen outside of the submitted work. CW-G reports grants from the Wellcome Trust during the conduct of the study. LS reports grants from United Kingdom Research and Innovation during the conduct of the study; grants from Wellcome, the UK Medical Research Council (MRC), the National Institute for Health Research (NIHR), GlaxoSmithKline, the British Heart Foundation, Diabetes UK, and the Newton Fund outside of the submitted work; and is a non-executive director of the Medicines and Healthcare Products Regulatory Agency. AG works for AstraZeneca outside of the submitted work. JKQ reports grants and personal fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Bayer, and Chiesi; grants from The Health Foundation and the MRC; and study funding from Asthma UK outside of the submitted work. MM is a member of Independent SAGE. SML reports grants from the Wellcome Trust, NIHR, MRC, and Health Data Research UK during the conduct of the study. All other authors declare no competing interests.
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Cookie settingsACCEPT
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.









{kind=link}