Key findings
- The national lockdown in Thailand was associated with a significant reduction in average daily ED visits across traumatic and non‐traumatic patients.
- Despite the decline in ED visits, the admission rates and ICU admission rates were increased.
- Although we could not conclude the cause of these changes, communication from healthcare professionals and public health officers is warranted to reinforce the importance of timely ED visits for acute health conditions.
Introduction
Since late December 2019, the severe acute respiratory syndrome coronavirus 2, which was subsequently identified as the cause of 2019 novel coronavirus disease (COVID‐19), became a disastrous threat to public health globally.1 Identified for the first time in Wuhan Municipal Health Commission, China, the severe acute respiratory syndrome coronavirus 2 began to spread rapidly across the globe.2 Thailand became the first country outside of China to report a confirmed case on 13 January 2020. Apart from the direct impact on death caused by COVID‐19, growing evidence demonstrates the negative consequences of this pandemic on health systems.3–6 Many countries imposed lockdown policies and restricted people’s movement, including social distancing, school closures and the interruption of non‐essential services. In Thailand, the government imposed the national lockdown from 26 March to 30 June 2020. The lockdown prohibited people from entering areas or places that are risk‐prone to the infection of COVID‐19 and instituted the curfew from 10 pm to 4 am.
The ED acts as a frontline in the pandemic’s response.7–9 Every patient, except those with an appointment, will generally be screened at the ED. The ED is also perceived as a hotspot for transmitting infection because of the high risk of exposure and the high number of personnel.8 Previous studies reported a significant reduction of up to 50% of ED visits during the 2003 SARS outbreak in Hong Kong and Taiwan.7, 9 Earlier this year, a national lockdown resulted in decreased ED attendance in several developed countries.10–13 This evidence suggests that people avoided ED visits for non‐coronavirus‐related illnesses and delayed their visits as long as possible because of the outbreak.14, 15 These might be a significant factor that increases the morbidity and mortality rate, especially those with life‐threatening conditions.15, 16 Evaluation of the impact from the COVID‐19 pandemic to the ED visits and admission rates could lead to better healthcare management systems for the future.
Thus, we investigated the impact of the COVID‐19 pandemic on ED visitation and admission rates to a university hospital in a developing country. We hypothesised that during the COVID‐19 outbreak and national lockdown, the total number of ED visits might decrease. Still, those who appear will present with late or more severe presentations, possibly because of less timely access to the ED.
Methods
This hospital‐based study was reported according to the Strengthening the Reporting of Observational Studies in Epidemiology statement.17
Study design and data collection
We conducted a retrospective cohort study in the ED at a single university hospital with approximately 30 000 ED visits annually. We performed an electronic medical database review of patients presenting to the ED during the national lockdown (between 26 March and 30 June 2020). A comparable control period was identified by retrieving patients’ data presenting to the ED during the same calendar period in 2019. Inclusion criteria included patients with non‐COVID‐19‐related problems presenting to the ED within the study and the control period. We excluded confirmed or suspected COVID‐19 patients. Specifically, we collected age, day and time of the visit, triage level, total ED time, type of disposition from the ED, code activation and invasive life‐saving procedures performed at the ED. For patients with incomplete data, we further reviewed each medical record to identify any missing information. Patients with unknown or unavailable data on essential items were excluded from the analysis.
Setting
In Thailand, the health system is based on universal health coverage, authorised under a National Health Security Act, B.E. 2545. Every emergency care is available for all individuals, including those without health insurance, enacted under an Emergency Medical Act, B.E. 2551. Maharaj Nakorn Chiang Mai Hospital is a university hospital which consists of 1500 patients’ bed, 151 intensive care unit (ICU) and sub‐ICU beds, 28 operating rooms and staff doctors of all subspecialties. Typically, the proportion of traumatic and non‐traumatic patients presenting to this ED is 1:1 and approximately 15% are screened as ‘Emergency’ level or above. The triage classification is based on a five‐level system, according to the Canadian Triage and Acuity Scale, ranging from blue (level 1, resuscitation) to white (level 5, non‐urgency). During the COVID‐19 outbreak, our hospital launched a new policy to handle this pandemic. Every patient presenting to the ED is screened by triage officers. Patients with positive or suspected COVID‐19 are isolated in prepared examination rooms. Our ED provides a 24‐h service with the presence of emergency physicians and experienced nurses.
In the present study, we classified seven types of disposition: ICU admission, general ward admission, observational unit admission, referral to another hospital, discharged, discharged against doctor’s advice and death. Our department has implemented several code activations to ensure that patients receive appropriate treatments in a timely manner. Code activations in the present study included sepsis/septic shock, ST‐elevation myocardial infarction (STEMI), stroke and severe head injury. The life‐saving procedures mentioned in the present study consist of tracheal intubation and cardiopulmonary resuscitation.
Ethical consideration
Patient confidentiality was preserved by using anonymous health records. The study was approved by the Institutional Review Board (Approval No. EME‐2563‐07565).
Outcomes and statistical analysis
The primary outcome was the incidence rate ratio (IRR) with a 95% confidence interval (CI) of the daily number of ED attendance. Secondary outcomes included the IRR with 95% CI of the total admission and ICU admission. We analysed the data using Stata 16 (StataCorp, College Station, TX, USA). For continuous variables, the mean and standard deviation was used for the description of normally distributed data. The median and interquartile range was used for non‐normally distributed data. For continuous data, we compared the differences between the two groups using an independent t‐test or rank‐sum test based on the data distribution. We presented a categorical variable using frequency and percentage and compared with χ2 or exact probability test as appropriate. Any P‐value of less than 0.05 was considered statistically significant.
Admission rates were calculated for each day in 2020 and 2019 by dividing the number of admissions by the total number of patients who visited the ED. Cumulative admission rates were subsequently derived by the cumulative sum of the admission rates and were visualised separately for bar charts each year. Generalised linear regression with link identity and Gaussian family was performed to model two regression lines, one for 2020 and the one for 2019, for cumulative admission rates and ICU admission rates. Wald test statistics were used to compare the slopes of the two regression lines.
Results
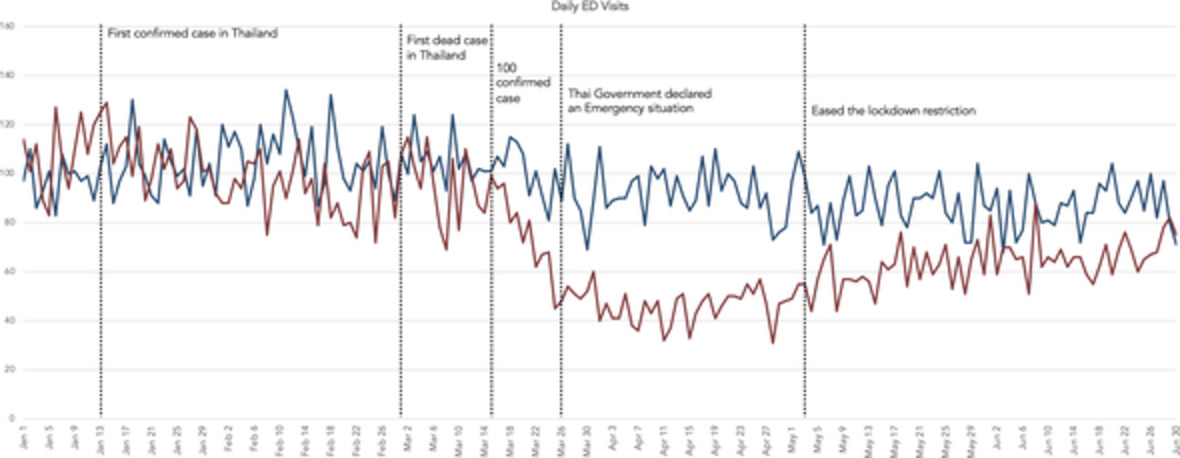
A total of 97 days in each period were reviewed. The average daily ED attendance in 2020 was 57.0 (95% CI 54.6–59.4), which decreased significantly compared to 2019 (89.1, 95% CI 87.1–91.1). The IRR of the average number of daily ED visits was 0.69 (95% CI 0.67–0.70). Despite the total declining number of cases, the proportion of patients whose triage levels were ‘Resuscitation’ and ‘Emergency’ increased in 2020 compared to 2019 (29.1% vs 19.2%, P < 0.001). Figure 1 demonstrates the number of daily ED visits since 1 January. The number of ED visits in 2020 began to fall after the total number of confirmed COVID‐19 cases in Thailand reached one hundred.

 ), 2019; (
), 2019; ( ), 2020.
), 2020.
During the COVID‐19 outbreak and national lockdown, the percentages of patients presenting to the ED during the day and the evening shift were increased. Conversely, the number of patients during the night shift markedly decreased (21.9% vs 30.7%, P < 0.001). Table 1 summarises the characteristics of patients presenting to the ED in 2019 and 2020. Overall, the patients who came to the ED during the COVID‐19 period were older than the previous year (median age 49 vs 38, P < 0.001). Yet, the percentages of patients who visited the ED during the weekdays were similar (71.3% vs 70.8%, P = 0.51).
Characteristics of patients presenting at the ED in 2019 and 2020
| Total | Non‐trauma | Trauma | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Exposure (2020) (n = 5529) | Comparator (2019) (n = 8644) | P‐value | Exposure (2020) (n = 3130) | Comparator (2019) (n = 4548) | P‐value | Exposure (2020) (n = 2399) | Comparator (2019) (n = 4096) | P‐value | |
| Age (mean ± SD) | 47.5 ± 35.6 | 43.0 ± 53.4 | <0.001 | 53.8 ± 42.5 | 49.4 ± 56.9 | <0.001 | 39.2 ± 21.3 | 36.0 ± 48.4 | 0.02 |
| Median age (IQR) | 49 (26–66) | 38 (22–62) | <0.001 | 58 (36–71) | 52 (25–68) | <0.001 | 35 (23–56) | 28 (21–50) | <0.001 |
| Day of visit – Weekday (n, %) | 3943 (71.3) | 6119 (70.8) | 0.51 | 2296 (73.4) | 3316 (72.9) | 0.68 | 1647 (68.7) | 2803 (68.4) | 0.87 |
| Time on arrival (n, %) | <0.001 | <0.001 | <0.001 | ||||||
| Day (08.01–16.00) | 2274 (41.1) | 3037 (35.1) | 1260 (40.3) | 1582 (34.8) | 1014 (42.3) | 1455 (35.5) | |||
| Evening (16.01–24.00) | 2042 (36.9) | 2953 (34.2) | 915 (29.2) | 1085 (23.9) | 1127 (47.0) | 1868 (45.6) | |||
| Night (00.01–08.00) | 1213 (21.9) | 2654 (30.7) | 955 (30.5) | 1881 (41.4) | 258 (10.8) | 773 (18.9) | |||
| Triage level (n, %) | <0.001 | <0.001 | <0.001 | ||||||
| Resuscitation | 425 (7.7) | 441 (5.1) | 344 (11.0) | 295 (6.5) | 81 (3.4) | 146 (3.6) | |||
| Emergency | 1181 (21.4) | 1221 (14.1) | 987 (31.5) | 1010 (22.2) | 194 (8.1) | 211 (5.2) | |||
| Urgency | 1770 (32.0) | 2650 (30.7) | 1283 (41.0) | 1955 (43.0) | 487 (20.3) | 695 (17.0) | |||
| Less urgency | 1666 (30.1) | 3380 (39.1) | 444 (14.2) | 917 (20.2) | 1222 (50.9) | 2463 (60.1) | |||
| Non urgency | 487 (8.8) | 952 (11.0) | 72 (2.3) | 371 (8.2) | 415 (17.3) | 581 (14.2) | |||
- IQR, interquartile range; SD, standard deviation.
During the COVID‐19 outbreak period, 3424 (61.9%) patients were discharged, 190 (3.4%) were referred to another hospital, 32 (0.6%) were discharged against doctor’s advice and 32 (0.6%) died; the remaining patients were admitted to the hospital (ICU, general ward and observational unit) where the rate of total admission (33.5%) was greater than that observed during the control period (28.3%, P < 0.001). The IRR for the admission rate was 1.18 (95% CI 1.11–1.26), and the IRR for the ICU admission rate was 1.35 (95% CI 1.21–1.52). Figures 2 and 3 demonstrated the cumulative admission rates and ICU admission rates compared between 2020 and 2019. From the modelling of cumulative admission rates, the regression slope for the year 2020 was +0.337 (95% CI 0.336, 0.339, P < 0.001), and the regression slope for the year 2019 was +0.290 (95% CI 0.289, 0.292, P < 0.001). For the cumulative ICU admission rates, the regression slope for the year 2020 was +0.103 (95% CI 0.102, 0.104, P < 0.001), and the regression slope for the year 2019 was +0.076 (95% CI 0.075, 0.077, P < 0.001). The P‐values for interaction based on Wald’s test showed statistically significant results (P < 0.001 for both models).

 ), 2019; (
), 2019; ( ), 2020.
), 2020.

 ), 2019; (
), 2019; ( ), 2020.
), 2020.
Our results also showed the differences in the percentage of code activation (Table 2). Noticeably, sepsis/septic shock code activation was decreased (1.6% vs 3.1%, P < 0.001), whereas STEMI and stroke code activation were increased (1.5% vs 1.0%, P = 0.007, 1.0% vs 0.7%, P = 0.03, respectively). We also observed an increased tracheal intubation rate during the COVID‐19 period (2.8% vs 1.8%, P < 0.001). Outcomes of patients presenting to the ED in 2019 and 2020, based on each time frame, were summarised in Table 2.
Outcomes of patients presenting at the ED in 2019 and 2020
| Total | Non‐trauma | Trauma | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Exposure (2020) (n = 5529) | Comparator (2019) (n = 8644) | P‐value | Exposure (2020) (n = 3130) | Comparator (2019) (n = 4548) | P‐value | Exposure (2020) (n = 2399) | Comparator (2019) (n = 4096) | P‐value | |
| Total ED time (min, mean ± SD) | 47 ± 24 | 54 ± 33 | <0.001 | 61 ± 27 | 78 ± 25 | <0.001 | 28 ± 251 | 28 ± 572 | 1.00 |
| Type of disposition (n, %) | <0.001 | <0.001 | 0.001 | ||||||
| ICU admission | 563 (10.2) | 650 (7.5) | 410 (13.1) | 436 (9.6) | 153 (6.4) | 214 (5.2) | |||
| General ward admission | 1065 (19.3) | 1353 (15.7) | 839 (26.8) | 1024 (22.5) | 226 (9.4) | 329 (8.0) | |||
| OU admission | 223 (4.0) | 443 (5.1) | 140 (4.5) | 235 (5.2) | 83 (3.5) | 208 (5.1) | |||
| Referred | 190 (3.4) | 241 (2.8) | 154 (4.9) | 173 (3.8) | 36 (1.5) | 68 (1.7) | |||
| Discharge | 3424 (61.9) | 5732 (66.3) | 1544 (49.4) | 2508 (55.1) | 1880 (78.4) | 3224 (78.7) | |||
| Against advice | 32 (0.6) | 187 (2.2) | 21 (0.7) | 145 (3.2) | 11 (0.5) | 42 (1.0) | |||
| Death | 32 (0.6) | 38 (0.4) | 22 (0.7) | 27 (0.6) | 10 (0.4) | 11 (0.3) | |||
| Code activation (n, %) | |||||||||
| Sepsis/septic shock | 91 (1.6) | 272 (3.1) | <0.001 | 91 (2.9) | 269 (5.9) | <0.001 | 0 (0) | 3 (0.1) | 0.30 |
| STEMI | 84 (1.5) | 87 (1.0) | 0.007 | 84 (2.7) | 86 (1.9) | 0.02 | 0 (0) | 1 (0.0) | 1.00 |
| Stroke | 57 (1.0) | 59 (0.7) | 0.03 | 57 (1.8) | 44 (1.0) | 0.001 | 0 (0) | 2 (0.0) | 0.53 |
| Severe head injury | 36 (0.7) | 63 (0.7) | 0.61 | N/A | N/A | N/A | 36 (1.5) | 63 (1.5) | 1.00 |
| Admission (n, %) | 1851 (33.5) | 2446 (28.3) | <0.001 | 1389 (44.4) | 1695 (37.3) | <0.001 | 462 (19.3) | 751 (18.3) | 0.36 |
| Intubation (n, %) | 154 (2.8) | 154 (1.8) | <0.001 | 129 (4.1) | 118 (2.6) | <0.001 | 25 (1.0) | 36 (0.9) | 0.51 |
| CPR (n, %) | 42 (0.8) | 45 (0.5) | 0.08 | 31 (1.0) | 27 (0.6) | 0.06 | 11 (0.5) | 18 (0.4) | 1.00 |
- CPR, cardiopulmonary resuscitation; ICU, intensive care unit; N/A, not applicable; OU, observational unit; SD, standard deviation; STEMI, ST‐elevation myocardial infarction.
Discussion
The present study demonstrated that the national lockdown was associated with a significant reduction in ED visits. This effect was demonstrated across traumatic and non‐traumatic patients. Despite the decline in ED visits, the admission rates and ICU admission rates were increased. Thailand was the first country to report a confirmed case of COVID‐19 outside of China on 13 January 2020. With COVID‐19 cases continuing to rise in Thailand and worldwide, several countries legislated national lockdown policies. The government of Thailand imposed the Public Administration in Emergency Situation decree from 26 March to 30 June 2020, which resulted in a drop in the daily number of patients presenting to the ED. This finding was consistent with the observations from several developed countries.10–12 For instance, in Melbourne, Australia, average daily ED attendance dropped from 278.8 to 174.7 presentations per day during State of Emergency restrictions.10 Deductions were evident across all triage levels and diagnostic categories, except for the most urgent patients. However, to our knowledge, this is the first documentation that highlights the association between reduced ED attendance and the implementation of a national lockdown in a developing country.
The primary determinant of the overall reduction in ED visits was fewer lower acuity presentations. Our study found that patients whose triage levels were ‘Less urgent’ and ‘Non‐urgent’ were decreased, which correlated with the findings from two EDs in Australia.10 Similar to a study concerning the SARS pandemic in 2003, the rate of ED attendance was reduced in Hong Kong during the outbreak.7 The reason for these markedly reduced numbers during the pandemic could be multifactorial.18 First, previous literature has mentioned the impact of fear of contacting COVID‐19 in the hospital. It has been reported that most of the patients delayed seeking emergency services.18–20 From the number of daily ED visits in our study, the downward trend began after the number of COVID‐19 positive in Thailand reached one hundred. This finding highlights this fear and that most people preferred to stay at home. Moreover, a national lockdown policy might frighten people from ‘going to the hospital’ because it was considered a hotspot for transmitting the virus.21 Second, the lockdown included closures of schools, restaurants, entertainment venues and other public places. These closures were associated with a significant reduction in contagious diseases via airborne and faecal‐oral transmission. Consistent with a time series analysis of six large EDs in France, COVID‐19 lockdown and school closures were associated with a significant decrease in paediatric infectious disease disseminated via airborne transmissions.22 Third, some researchers proposed that the reduction of daily physical activities might correlate with the deduction chances of patients with acute exacerbations of pulmonary and cardiovascular emergencies.23, 24 Last, almost all hospitals, including our institute, cancelled elective surgeries and this may have resulted in fewer ED visits because of iatrogenic or post‐operative complications.
Despite a total decline in ED visits, we also found that both overall admission rates and ICU admission rates increased during the pandemic. However, the proportions of admissions might increase because of an increase in the high acuity patients’ ratio. Consistent with the findings from Cuneo, Italy, these changes have been mentioned.24 The proposed reason included the rising in ‘questionable use of the EDs’; patients with self‐limiting conditions would not come to the EDs unless necessary.24 Although there was an increase in STEMI and stroke activation, sepsis/septic shock activation in the present study decreased surprisingly during the pandemic. STEMI and stroke have unique and specific presentations and symptoms. Patients with STEMI typically have chest pain, and patients diagnosed with stroke will generally come to the ED complaining of weakness. Previous literature described the significant changes in daily clinical practice, including stroke and myocardial infarction.15, 25, 26 Unfortunately, patients with sepsis/septic shock might not realise whether they already have this illness or not because sepsis/septic shock has a wide range of severity and various symptoms that could be presented.27 These findings could enhance the issue of uncertainty in accessing the ED. Additionally, we further reviewed the incidence of COVID‐19 confirmed cases in our hospital, which may correlate with the declining number of sepsis/septic shock activation. Until 31 July 2020, our hospital had a total of eight confirmed cases, which were remarkably low compared to total cases of sepsis/septic shock activation. This finding could emphasise the importance of public education about the clinical presentations of sepsis/septic shock. Therefore, proper education and timely access to the ED should be warranted to minimise the impact of COVID‐19 and the national lockdown on sepsis/septic shock outcomes.
The findings of the present study provide some important implications. They focus on the possibility that some patients are delaying medical evaluation in the ED. Although the national lockdown directly restricted people’s transportations, which resulted in a decreasing number of traumatic patients, our study has pinpointed the declining number of non‐traumatic patients as well.
Overall, the present study adds to the emerging body of literature regarding the impact of the pandemic and gives a valuable international perspective. Thailand might be one of the best COVID‐19 management countries28 however, the indirect effect regarding this pandemic, for example, the impact of COVID‐19 on non‐COVID‐19‐related conditions and ED administration, needs to be addressed.29
Limitations
There were some limitations in our study. Despite comparing two periods in the same calendar time, this approach could not account for underlying trends in ED attendance. Changes in ED attendance patterns might incidentally associate with the pandemic or the restrictions. Further time series analysis or regression modelling over a more extended period would address this issue. Second, we conducted the study only in one university hospital. Thus, the design might be valid and generalisable to the setting within the same level of care. Maharaj Nakorn Chiang Mai represented a tertiary care hospital; it is also subject to the risk of referral bias. Third, every hospital in the world was dealing with this outbreak in different conditions because of its novelty and lack of reliable evidence on the best management guidelines. Our hospital has implemented a policy to distinguish COVID and non‐COVID‐related ED visits. Yet, it was challenging to identify all of the ED visits accurately. Besides, the present study did not include data on the changes in the frequency of presentation for different diagnostic groups. We collected only the code activations in the ED, including significant illnesses and time‐sensitive diseases. Finally, our study served as an observational study which could not conclude all of the causes that impact the decline in ED access. To properly imply these causations, prospective and population‐based studies are required. Also, a qualitative study focusing on patients’ perceptions towards the lockdown is necessary to reduce preventable outcomes resulting from delayed access to emergency medical services.
Conclusion
To conclude, COVID‐19 affects not only normal daily life but also in the healthcare system.
The present study highlights the changes in the frequency and pattern of ED presentations. Restrictions regarding to handle this outbreak were associated with a significant reduction in average daily ED visits across traumatic and non‐traumatic patients. Although we could not conclude the cause of these changes, communication from healthcare professionals and public health officers is warranted to reinforce the importance of timely ED visits for acute health conditions and assure the public that EDs are administering infection prevention to ensure the safety of both patients and healthcare personnel.
Acknowledgement
The authors gratefully acknowledge Mr Jonathan Bostwick for an elaborative language editing on our manuscript.
Author contributions
WW, TS, WY, PP conceived the study and designed the study. WW and WY contributed to data collection. WW and PP performed the data analysis. WW drafted the initial article. All authors read and approved the latest version of the manuscript.
Competing interests
None declared.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References







{kind=link}